-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(11): 2874-2878
doi:10.5923/j.ajmms.20241411.42
Received: Oct. 23, 2024; Accepted: Nov. 13, 2024; Published: Nov. 15, 2024

On the Problem of Treatment and Diagnostic Algorithm for Acute Appendicitis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSh. A. Tadzhibaev1, E. K. Sobirov2, F. Sh. Abdurashidov1
1Andijan State Medical Institute, Andijan, Republic of Uzbekistan. (Rector, Doctor of Medical Sciences, Prof. Madazimov M.M.)
2ALMOZN Medical Hospital, (Hospital Director Dr Ali Alejenef), Zintan, Arab Republic of Libya
Correspondence to: Sh. A. Tadzhibaev, Andijan State Medical Institute, Andijan, Republic of Uzbekistan. (Rector, Doctor of Medical Sciences, Prof. Madazimov M.M.).
| Email: |  |
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Relevance: Dynamic progress in abdominal surgery, based on the development of non-invasive and minimally invasive diagnostic and treatment technologies, dictates the need to create an effective diagnostic and treatment algorithm that makes it possible to simultaneously solve the problem of diagnosis and treatment of acute appendicitis. Aim- To develop a diagnostic and treatment algorithm for acute appendicitis for a combined solution to the problems of diagnosis and surgical treatment of acute appendicitis based on the capabilities of non-invasive and minimally invasive technologies. Materials and methods: The study is based on an analysis of observations of 128 patients with acute appendicitis and its complications who underwent appendectomy using endovideolaparoscopic technique. The age of the patients ranged from 16 to 64 years. Men – 71 (55.5%), women – 57 (44.5%). Ultrasound examination (ultrasound) was performed using a SonoScape – P20 scanner, manufactured in Germany. According to indications, multislice computed tomography (MSCT) on a tomograph made in the USA, General Electric, model 2022. Surgical interventions were performed with an endovideolaparoscopic complex from COMEG, manufactured in Japan, and a set of instruments from Karl Storz, manufactured in Germany. Results: The sensitivity of ultrasound for acute appendicitis was 87.6%. In 123 patients, at the stage of diagnostic laparoscopy, the diagnosis was not in doubt, that is, the diagnostic accuracy of endovideolaparoscopy for acute appendicitis was 96%. Of the 128 patients, 22 (17.2%) were diagnosed with a catarrhal form, 89 (69.5%) patients with a phlegmonous form, and 17 (13.3%) with a gangrenous form. In the group with destructive forms -106 (82.8%) in 7 (6.6%) cases, appendictomy was performed extracorporeally with a minimal degree of traumatic open access, but sanitation and drainage were performed laparoscopically. In the early postoperative period, suppuration occurred at the point of insertion of the umbilical trocar in 6 (4.7%) patients. Conclusions: The use of a diagnostic and treatment algorithm optimizes the diagnosis of acute appendicitis and its complications, shortens the preoperative diagnostic period, specifies the indications for surgical treatment, expands the range of choice of an adequate surgical option, it is possible to simultaneously solve the problem as a diagnosis, and treatment, which generally improves the results of surgical treatment of acute appendicitis and its complications.
Keywords: Acute appendicitis, Diagnostic videolaparoscopy, Laparoscopic appendectomy
Cite this paper: Sh. A. Tadzhibaev, E. K. Sobirov, F. Sh. Abdurashidov, On the Problem of Treatment and Diagnostic Algorithm for Acute Appendicitis, American Journal of Medicine and Medical Sciences, Vol. 14 No. 11, 2024, pp. 2874-2878. doi: 10.5923/j.ajmms.20241411.42.
- The study was carried out within the framework of scientific theme No. 012000267 “Development of advanced technologies in the diagnosis, treatment and prevention of acute surgical diseases of the abdominal organs”, Andijan State Medical Institute. The study has no sponsorship.
1. Relevance
- The dynamic progress of modern abdominal surgery, based on the introduction of medical technology achievements and, accordingly, the development of non-invasive and minimally invasive diagnostic and treatment technologies, dictates the need to create an effective therapeutic and diagnostic algorithm that combines the capabilities of all methods into one single whole and makes it possible to simultaneously solve the problem of diagnosis and treatment. This problem covers all urgent abdominal surgery in general and the problem of diagnosis and treatment of acute appendicitis and its complications in particular. This requirement is associated with the frequency of occurrence, which is 22.8 per 10,000 population [1,2], a high incidence of 4-6%, appendectomies account for about 40% of all operated urgent patients, in addition, the number of errors at stages diagnosis of acute appendicitis without use cases modern non-invasive and minimally invasive methods diagnostics services, it reaches up to 31% [3]. Diagnosis of acute appendicitis in atypical and rare forms is particularly difficult [4], and it should be taken into account that 4-42% of patients have complicated appendicitis [5], and every year in the world from 50 to 70 thousand people die from acute appendicitis and its complications. a person [6]. In addition, according to the data of the Chief Surgeon of the Ministry of Health of Russia A. Sh. According to Revishvili, 148,763 patients diagnosed with Acute appendicitis were treated in the Russian Federation in 2022, and surgical activity in 2020 was 98.1%, mortality-0.17% [7]. All these data together emphasize the urgency of the problem.It is generally accepted that if there are differential diagnostic difficulties in acute appendicitis, diagnostic laparoscopy should be performed. As for surgical treatment, since 1983, laparoscopic appendectomy has gained wide popularity, and up to 75% of operations are performed laparoscopically in the world. Moreover, some authors advocate granting laparoscopic appendectomy the status of the "gold standard" for surgical treatment of acute appendicitis [8]. At the same time, although in Russia the role of laparoscopic technologies in the surgical treatment of acute appendicitis tends to increase, the frequency of their use remains low and amounts to 27% [9]. In addition, the use of laparoscopic access in the treatment of acute appendicitis, in particular complicated by advanced appendicular peritonitis, is still a controversial issue [10,11].Problematic issues related to acute appendicitis are unified in the National Clinical Guidelines (NCR) and international recommendations of various surgical societies – the World Community for Emergency Surgery (WSES), European Association of Endoscopic Surgeons (EAES) [12]. Issues related to the definition of tactical approaches to complex clinical situations that arise in acute appendicitis were debatable during the NCR discussions [13]. Thus, the development and creation of an effective yet compact treatment and diagnostic algorithm for acute appendicitis, taking into account the capabilities of modern non-invasive and minimally invasive technologies, which makes it possible to simultaneously solve the problem of diagnosis and treatment, is relevant and timely. At the same time, it should be noted that acute appendicitis is primarily a clinical diagnosis [14], and the clinical manifestations of this pathology, together with the results of diagnostic methods, determine the vector of patient management and treatment.Research objective: To develop a therapeutic and diagnostic algorithm for acute appendicitis for the combined solution of problems of diagnosis and surgical treatment of acute appendicitis based on the capabilities of non-invasive and minimally invasive technologies.Tasks: Based on our own clinical material to analyze the results of non-invasive and minimally invasive methods of diagnosis and treatment of acute appendicitis and its complications, to identify the effectiveness of these methods and determine the sequence of their application in order to develop a therapeutic and diagnostic algorithm.
2. Materials and Methods
- Based on the Department of Surgery of a Medical hospital ALMOZSo, from 2019 to 2024, 182 patients underwent surgery for acute appendicitis using endovideolaparoscopic techniques. This work is based on the analysis of observations of 128 patients with acute appendicitis and its complications who underwent appendectomy using endovideolaparoscopic techniques, 54 (29.7%) patients out of 182, the technique of performing operations had its own characteristics and they are the object of our further research. The age of the patients ranged from 16 to 64 years. Men – 71 (55.5%), women – 57 (44.5%). All patients underwent a comprehensive examination, while the basic ones were anamnesis collection, clinical and laboratory examination, ultrasound examination of the abdominal cavity, and diagnostic laparoscopy (DL). Ultrasound examination of the abdominal cavity was performed using a scanner SonoScape – P20, manufactured in Germany. Multispiral computed tomography (MSCT) is indicated. This study was performed on a CT scanner manufactured in the USA, General Electric, model 2022. Diagnostic laparoscopy and surgical interventions were performed using the company's endovideolaparoscopic complex COMEG, made in Japan, and a set of Ka toolsrl Storz manufactured in Germany. Histological studies were conducted at the Attasami Diagnostic Services Diagnostic Center, Tripoli, Libya. Statistical processing of the material included the calculation of extensive indicators.
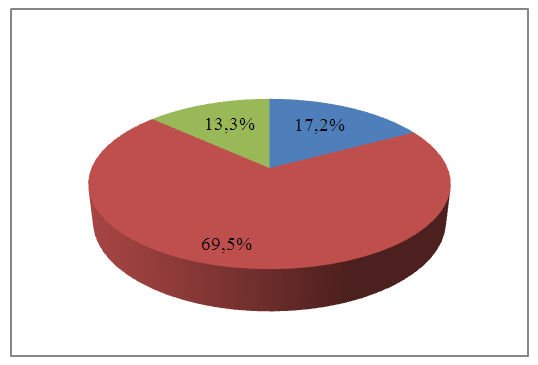 | Figure 1. Distribution of patients by pathomorphological diagnosis |
3. Results and Discussion
- A thorough analysis of the available clinical material revealed a certain sequence of treatment from the moment of admission to discharge of patients. The first stage was a general clinical examination, which was carried out in the classic version.The next stage of the examination was the use of ultrasound examination of the abdominal cavity. Normally, the appendix is not visualized, so the very fact of visualization of the appendix indicates its inflammation. Direct ultrasound signs of acute appendicitis were an increase in the diameter of the appendix to 8-10 mm or more (normally 4-6 mm), thickening of the walls to 4-6 mm or more (normally 2 mm), which in cross-section gives a characteristic symptom of "target" ("cockades"). With gangrenous-perforated appendicitis, the contents of the process pour out into the abdominal cavity, dilatation disappears, and the process may not be located. It should be noted that the sensitivity of ultrasound examination in acute appendicitis was 87.6%. The results of this study show that accurate diagnosis of this method is directly proportional to the destructive changes in the appendix.One of the methods of noninvasive diagnosis of acute appendicitis used by us was multislice computed tomography (MSCT) – 43 patients. In 28 cases, i.e. 65.1%, signs of acute appendicitis were diagnosed, in 15(34.9%) patients, acute appendicitis was excluded. These figures show the effectiveness of the method. Indications for this study were difficult-to-diagnose cases, to exclude somatic pathology simulating acute diseases of the abdominal cavity. On tomograms of acute appendicitis, signs of appendix inflammation were: Thickening of the wall (more than 3 mm), inflammation of the appendix membranes, peri-intestinal effusion around the cecum or adipose tissue infiltration, which were pathognomonic signs of acute appendicitis.The initial stage of surgical intervention was diagnostic videolaparoscopy, which was performed through an 11-mm trocar installed at the top of the Tracing Paper. For a complete visual revision, a second 5 - mm trocar for the manipulator was installed along the midline 3-4 cm below the navel, depending on the situation, taking into account that if signs of appendicitis were detected, it was possible to perform a laparoscopic appendectomy. Direct signs were visible changes in the process, rigidity of the walls, hyperemia of the visceral peritoneum, small-point hemorrhages on the serous cover of the process, fibrin overlays, mesentery infiltration. Indirect signs: the presence of a cloudy effusion in the abdominal cavity (most often in the right iliac fossa and pelvis), hyperemia of the parietal peritoneum in the right iliac region, hyperemia and infiltration of the cecum wall.Specific signs of catarrhal appendicitis, which allow us to distinguish it during laparoscopy from secondary changes in the process, were not detected against the background of another pathology. In each specific case, the issue of performing an appendectomy was decided individually, taking into account the clinic, the results of other research methods, and the operating situation.With phlegmonous appendicitis, the process is thickened, tense, the serous membrane is hyperemic, has hemorrhages, fibrin deposits. The mesentery is infiltrated, hyperemic. There is a cloudy effusion in the right iliac region. In gangrenous appendicitis, the process is sharply thickened, greenish-black in color, unevenly colored, fibrin overlaps on its serous membrane, and the mesentery is sharply infiltrated (Fig. In 123 patients at the stage of diagnostic laparoscopy, the diagnosis of acute appendicitis was not in doubt, that is, the diagnostic accuracy of endovideolaparoscopy in acute appendicitis was 96%.
 | Figure 2 |
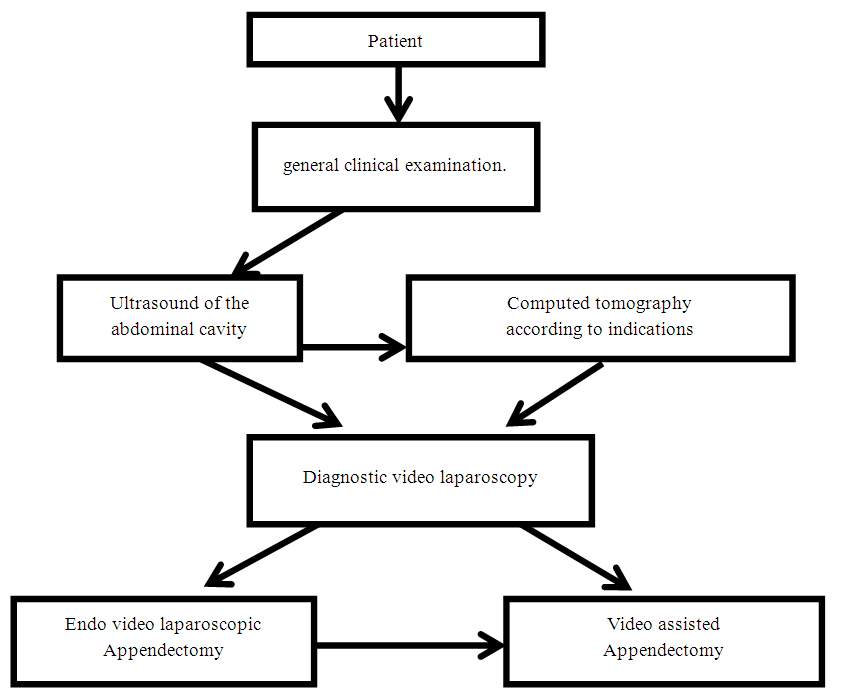 | Figure 3. Therapeutic and diagnostic algorithm for acute appendicitis |
4. Conclusions
- The results of non-invasive and minimally invasive diagnostic methods showed that the sensitivity of ultrasound examination in acute appendicitis was 87.6%, the exact diagnosis of this method is directly proportional to the destructive changes in the appendix. In 123 patients out of 128 at the stage of diagnostic laparoscopy, the diagnosis of acute appendicitis was not in doubt.The surgical accuracy of endovideolaparoscopy in acute appendicitis was 96%.These data prove the need to introduce non-invasive and minimally invasive diagnostic methods, namely ultrasound and diagnostic endovideolaparoscopy, into the program of the treatment and diagnostic algorithm for acute appendicitis. The use of videolaparoscopic techniques in the complex diagnosis of acute appendicitis will make it possible to transfer diagnostic endovideolaparoscopy to the therapeutic category when confirming the diagnosis.The use of the therapeutic and diagnostic algorithm makes it possible to optimize the diagnosis of acute appendicitis and its complications, shorten the preoperative diagnostic period, specify indications for surgical treatment based on the results of non-invasive and minimally invasive diagnostic methods, and expand the possibility of choosing an adequate surgical intervention option. In addition, it is also possible to simultaneously solve the problem, both diagnosis and treatment. All this generally improves the results of surgical treatment of acute appendicitis and its complications.