-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(11): 2810-2814
doi:10.5923/j.ajmms.20241411.28
Received: Oct. 15, 2024; Accepted: Nov. 7, 2024; Published: Nov. 12, 2024

Effect of Physical Activity on Intradialysis Vascular Dysfunction
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLM. A. Sabirov1, A. B. Daminov2, N. N. Sultonov1
1Republican Scientific and Practical Medical Center of Nephrology and Kidney Transplantation, Tashkent, Uzbekistan
2Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan
Correspondence to: M. A. Sabirov, Republican Scientific and Practical Medical Center of Nephrology and Kidney Transplantation, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

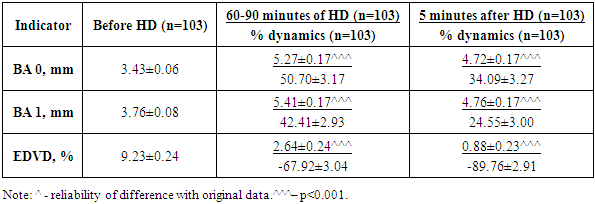
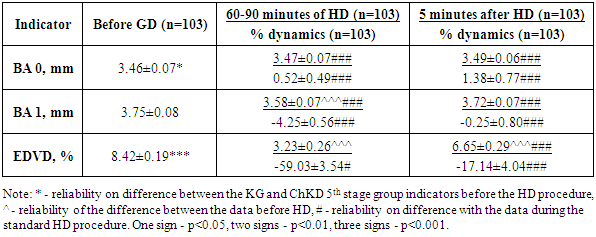
The article presents a study of intradialytic dynamics of endothelium-dependent vasodilation with the use of intradialytic physical exercise. Total of 103 patients with Chronic kidney disease ChKD 5th stage and 20 healthy volunteers of the corresponding age were studied. All study participants underwent instrumental examination, including a study of the functional state of the endothelium. In patients with ChKD 5th stage, compared with healthy individuals, there is a violation of the functional state of the endothelium, confirmed due to reduction to the degree of endothelium-dependent vasodilation (EDVD) (9.23±0.24% vs 12.90±0.25%, p<0.001). Hemodialysis is associated with further deterioration of the vasoactive function of the endothelium (decrease in EDVD to 2.64%) by 60-90th minute. Intradialytic physical exercise has a protective effect in terms of progression of endothelial dysfunction by 60-90th minute of dialysis: tendencies towards normalization of EDVD by the end of the hemodialysis (HD) session.
Keywords: Hemodialysis, Endothelium-dependent vasodilation, Intradialytic exercise
Cite this paper: M. A. Sabirov, A. B. Daminov, N. N. Sultonov, Effect of Physical Activity on Intradialysis Vascular Dysfunction, American Journal of Medicine and Medical Sciences, Vol. 14 No. 11, 2024, pp. 2810-2814. doi: 10.5923/j.ajmms.20241411.28.
Article Outline
1. Introduction
- During hemodialysis, the body is exposed to many factors, the adverse effects of which are potentiated by the high rate of change. In fact, patients with ChKD 5th stage are under the constant influence of stress, which can be classified into 2 time phases: the acute phase during the hemodialysis procedure, during which there is a rapid decrease in the volume of circulating plasma and cardiac output [1], a shift in the electrolyte status [2], a decrease in the concentration of amino acids and other small molecules in the blood plasma, activation of complement and systemic inflammation with the accumulation of proinflammatory cytokines [3], thermal shift [4], hemolysis, and transport of pyrogens [5]; and the second chronic phase, which occurs during the interdialytic period, during which there is an accumulation of fluid and uremic toxins in the body [6], and metabolic acidosis develops [7]. The negative impact of both phases of hemodialysis stress is enhanced by hypoxia [8] caused by pulmonary hypertension and chronic anemia. Intradialytic biochemical changes, fluctuations in osmotic pressure, acid-base and water-electrolyte balance are defined as dialysis imbalance syndrome [9,10].Endothelial cells are barrier formations that are primarily affected by the factors described. Acute hemodialysis stress contributes to the disruption of the structural and functional state of the endothelium due to the influence of stress factors on the cell membrane (reduction in plasma volume, thermal stress, accumulation of cytokines), decrease in the mitochondrial reserve (hypoxia, decreased glucose concentration), plastic deficiency - decrease in the concentration of amino acids, dystrophy - a violation of the acid-base balance. Endothelial dysfunction is primarily manifested by a shift in the expression of vasodilating and vasoconstrictor factors in favor of the latter, as well as a violation of the basal production of vasodilators. In addition, the bioavailability of nitric oxide decreases due to its binding to free hemoglobin formed during hemolysis, and the effect of endothelin-1 increases, since endothelin-1 binds to type A receptors, the activation of which potentiates vasoconstriction, and type B receptors, the activation of which potentiates vasodilation through the activation of Nitrous Oxide System (NOS), but in ChKD conditions, due to the blockade of nitric oxide, this effect is practically not manifested [11,12]. Vasculopathy in patients with ChKD 5th stage is caused not only by endothelial dysfunction and impaired response of vascular wall smooth muscle cells to vasodilating endothelial stimuli due to decrease in the number of myocytes and fibrosis and calcification of the wall [13,14,15].The structural and functional state of the endothelium can be assessed both of them during functional tests and based on the results of laboratory research. To assess the endothelial vasomotor function, a compression test is used, based on the change in diameter of brachial artery after 5-minute compression of brachial artery. Compression of brachial artery causes hypoxia of peripheral part of the limb and vasodilation due to accumulation of under oxidized products. After removal the compression, the high-speed blood flow displaces glycocalyx on the surface of endotheliocytes, causing shear stress. The shift of the glycocalyx deforms receptors - protein molecules located on the membrane and immersed with their outer end in the glycocalyx. A change in the conformational structure of the protein activates intracellular signaling pathway and causes the expression of nitric oxide. This process can be assessed by the degree of change in the diameter of the artery - in case of healthy vessels, the diameter of the brachial artery should increase more than 10% original. In case of violation of endothelium-dependent vasodilation, insufficient increase in diameter or even paradoxical vasoconstriction may be observed.Therapeutic interventions to prevent intradialytic vascular dysfunction may include changes in hemodialysis regimen - intensive nocturnal hemodialysis, change of dialysate, use of dialysate membranes with modified surface properties, but this approach is associated with financial and logistical difficulties, in addition, does not has a sufficient evidence base yet. The use of drugs aimed at normalizing the functional state of the endothelium - levorotatory arginine is debatable, since patients with CKD have a systemic inflammatory reaction accompanied by activation of macrophage NO synthase, which calls into question the effectiveness of drugs that release nitric oxide [16]. Another group of drugs with proven endothelial efficacy - statins, have no point of application in CKD, since they are absorbers, not synthetics of cholesterol, in addition, in patients with CKD, cholesterol has a cytostatic effect on effectors of inflammation [17].A possible option for the effect may be dynamic physical activity, which promotes normalization of the functional state of endothelium [18]. Dynamic physical activity also promotes effective transition of extracellular fluid into the lumen of vessels and the minimization of intradialytic hypotension [19,20]. Effect of physical activity on the functional state of the vascular wall in patients with CKD requires a detailed study, including an assessment in various mechanisms.Purpose of the study– to study the intradialytic dynamics of endothelium-dependent vasodilation when using intradialytic physical exercise.
2. Material and Research Methods
- The present study included 103 patients with ChKD 5th stage and 20 healthy volunteers in corresponding age. All study participants signed informed consent and received explanations about the importance of physical activity in maintaining health and treatment tactics, as well as the complexity of pathophysiological changes associated with the terminal stage of ChKD and HD.All study participants underwent instrumental examination, including a study of the functional state of the endothelium. The data obtained in the group of patients with ChKD 5th stage (103 people) were compared with the data obtained in the group of healthy volunteers (CG, 20 people).All patients with ChKD 5th stage included in the study were examined during 2 HD sessions, each after 3-day break. The first session was conducted using the standard technique for the patient. Before the session (standard HD 0), during the session at 60-90 minutes of HD (standard HD1) and after the end of HD (standard HD2), patients underwent serial Doppler sonography of brachial artery (BA) with determination of EDVD. The second HD session was conducted using intradialytic physical activity PA for 30 minutes of the first hour of HD. Serial examinations were conducted according to the above-described scheme.During the study, the intradialytic dynamics of pathophysiological changes under study were studied, the dynamics were compared against the background of standard HD and HD with PA, as well as depending on the age of the patients participating in the study.The study included individuals aged 18-70 years with ChKD 5th stage of various etiologies, aware of nature disease, the effects and risks of physical activity, and who gave consent to participate in the study. The criteria for non-inclusion in the study were: the presence of pathology limiting physical performance or terminal organ failure, except for ChKD, malignant tumors, fever, acute period of infectious diseases or exacerbation on chronic diseases affecting performance and quality of life, incapacity of the patient or refusal of the patient to participate in the study.The majority of patients included to the study fell into the 40-49 age group, slightly less often into the 30-39 age group. By etiology, most patients developed CKD due to chronic glomerulonephritis (36 people) and type 2 diabetes (33 people). By the duration of HD, all patients were evenly represented in 3 categories: up to 6 months, 6-12 months and 12-24 months.Endothelium-dependent vasodilation test (EDVD) of brachial artery (BA). Test is based on duplex scanning the BA contralateral to the AV fistula. An ultrasound scanner equipped with a linear sensor with a frequency of 7.5-10 Hz was used. The BA was scanned 2 cm above the elbow bend, the diameter of the artery (PA 0) was measured. Then a tonometer cuff was applied over scanning site, inflated to 50 mm Hg above the systolic blood pressure and fixed for 5 minutes. After 5 minutes, the cuff was removed and 60 seconds after removal compression, the BA was re-located and diameter (PA1) was determined. The relative dynamics of BA during the test was taken as a degree of EDVD of BA.Intradialytic exercise was used as an intervention, the effectiveness in which was studied in the course of this study. For this purpose, a portable exercise machine designed for pedaling with hands or feet in a sitting or lying position was used. The load was carried out for 30 minutes in first hour from the beginning of HD. Most patients used foot pedaling with a resistance 25 W and pedaling speed of 60 rpm. In case of lower limb muscle atrophy, low-intensity load was used - without resistance and at speed of 30 rpm. In case of gangrene, amputation of the foot/part of the foot, trophic ulcers, severe painful form peripheral neuropathy, hand pedaling without resistance at speed of 60 rpm was used.All data obtained in the course on this study were entered into summary tables on the Excel for Windows editor with subsequent sorting into groups in accordance with a purpose and objectives of the study. In the case of parametric data subject to normal distribution, arithmetic means and their standard errors were calculated to the groups, intergroup comparison was performed using the unpaired Student's criterion. In case of nonparametric features, their frequency was determined and intergroup comparison was performed using the chi-square table criterion and an assessment of its reliability according to the tables, taking into account number in degrees of freedom. The dynamics indicators in the groups was calculated as an average value of relative dynamics of indicators for all group participants, the reliability in the dynamics was determined using the paired Student's criterion.
3. Research Results and Discussion
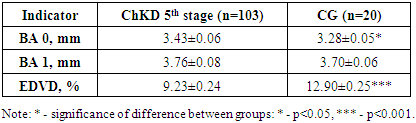
- The study of 103 patients receiving programmed hemodialysis at the Republican Scientific and Practical Medical Center of Nephrology and Kidney Transplantation, (during the 2nd hour of HD) and after the HD procedure, carried out after 3-day break. The concentration of creatinine in the main group of patients was 665.89±13.47 μmol/l vs. 67.70±1.85 μmol/l in the CG (p<0.001) and did not differ depending on the age of patients (670.69±20.04 μmol/l in patients under 41 years old and 661.24±17.69 μmol/l, p>0.05) and the etiology of ChKD (668.55±28.37 μmol/l in patients with diabetes and 656.35±12.91 μmol/l in patients with non-diabetic etiology of ChKD, p>0.05).The study of the state of endothelium-dependent vasodilation was carried out during the test with a 5-minute cuff compression of brachial artery(BA), during which the diameter of brachial artery was measured before compression and 1 minute after removing the cuff and restoring blood flow (Table 1). During the study, it was found that in patients with ChKD 5th stage the diameter of brachial artery was significantly larger than in representatives of the CG (p < 0.05). After removing the compression, diameter of BA increased both in the CG and in the group of patients with ChKD 5th stage, but the dynamics were significantly smaller in the main group of the study (p < 0.001 reliability of the difference in relative dynamics between the ChKD 5th stage and CG groups), as a result, by the 1st minute after removing compression of the BA, the diameter of BA was comparable in both groups of the study. Thus, in 77 representatives of the ChKD 5th stage group (74.76%), the EDVD was less than 10% and only in 26 (25.24%) was it 10% or higher.
|
|
|
4. Conclusions
- In patients with stage 5 CKD, compared with healthy individuals, there is a violation of functional state of the endothelium, a reliable decrease in degree of endothelium-dependent vasodilation (9.23 ± 0.24% versus 12.90 ± 0.25%, p < 0.001). Hemodialysis is associated with further deterioration of the vasoactive function of the endothelium (a decrease in the EDVA to 2.64%) by 60-90th minute. By the end of HD, endothelial dysfunction continues to progressively increase, the EDVA decreases to 0.88%. According to study results, intradialytic endothelial dysfunction is more pronounced in individuals under 41 years of age compared to older individuals. Intradialytic physical activity had protective effect in terms of the progression of endothelial dysfunction already by 60-90th minute of dialysis: there was tendency for the EDVA to normalize by the end of the HD session.