Ruziev U. U.1, Abdurakhmanov M. M.2
1Bukhara Branch of the Republican Scientific Center for Emergency Medical Care, Bukhara, Uzbekistan
2Department of Surgical Diseases, Bukhara State Medical Institute named after Abu Ali ibn Sino, Bukhara, Uzbekistan
Correspondence to: Ruziev U. U., Bukhara Branch of the Republican Scientific Center for Emergency Medical Care, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
To find new ultrasound signs of acute cholecystitis during color duplex scanning (CDS) of the gallbladder (GB). The gallbladder was examined using color duplex scanning (CDS) in 272 patients with acute calculous cholecystitis (ACC) with comorbid cardiovascular diseases in order to find additional signs to the known ultrasound signs of the disease. Also, at the first stage, 60 healthy volunteers were examined as a control group. The conducted analysis of the studies showed the greatest significance in the diagnosis of the disease of an increase in the maximum systolic velocity (Vmax) of blood flow in the branches of the cystic artery in the wall of the gallbladder. The results of the study showed that the use of ultrasound color duplex scanning as a non-invasive method allows determining the morphological form of acute cholecystitis and the presence of a destructive process in the gallbladder, which is important when making informed decisions about the need for surgical intervention.
Keywords:
Ultrasound diagnostics, Dopplerography, Color duplex scanning, Blood flow in the gallbladder wall, Acute cholecystitis
Cite this paper: Ruziev U. U., Abdurakhmanov M. M., Color Duplex Scanning of Blood Flow in the Gallbladder Wall in Acute Cholecystitis in Patients with Concomitant Cardiovascular Diseases, American Journal of Medicine and Medical Sciences, Vol. 14 No. 11, 2024, pp. 2726-2729. doi: 10.5923/j.ajmms.20241411.10.
1. Introduction
Ultrasound examination (US) plays an important role in the diagnosis and choice of treatment tactics for acute cholecystitis (AC) [1,2,3,8]. Characteristic signs of the disease in B-mode are changes in the size, thickness and structure of the gallbladder wall [2,7]. Also, generally recognized signs of AC, along with the ultrasound picture of the gallbladder in B-mode, are Doppler parameters of increased blood flow in the gallbladder wall by the type of arterial or venous hyperemia [9,10]. The data of Doppler examination of blood flow in the gallbladder wall in AC in patients with concomitant cardiovascular diseases (CVD) are contradictory [4,5,10]. The possibilities of ultrasound diagnostics of the biliary tract based on B-mode and using new technologies are discussed in a number of studies [9,11,13].The aim of our study was to search for new ultrasound signs of acute cholecystitis in patients with concomitant cardiovascular diseases, during color duplex scanning (CDS) of the gallbladder (GB).
2. Materials and Methods
We conducted a study of the gallbladder using the color duplex scanning (CDS) method in 272 patients of the main group with acute cholecystitis (ACC) 272 with comorbid cardiovascular diseases in order to search for additional signs to the known ultrasound signs of the disease.At the first stage of the study, 60 healthy volunteers were examined as a control group. We supplemented the comprehensive ultrasound examination of the gallbladder with ultrasound color duplex scanning of the vessels of its wall. The gallbladder was scanned in various planes - sagittal (longitudinal), transverse, frontal. Visual and quantitative analysis of the parameters was carried out based on generally accepted approaches.All of them had a visible color signal from the cystic artery in the gallbladder wall on color duplex scanning and were used for comparison with the blood flow data in the gallbladder vessels in patients with AC and comorbid CVD. The average age of the control group participants was 57.7 ± 3.4 years, and there was a predominance of women - 36 (60%) healthy individuals.
3. Results and Discussion
The average values of blood flow indices in the cystic artery were determined among all participants in the control group for comparison with the main study group (Table 1). The use of standard values of the gallbladder parameters and blood flow indices in its wall in healthy individuals allows them to be compared with the data of patients in the main study group.Table 1. Average blood flow rates of a. cystica in the gallbladder wall in the control group of healthy individuals
 |
| |
|
Ultrasound duplex scanning of the gallbladder wall vessels (USDS) was performed on 272 (100%) patients in the main group to clarify the nature of the inflammatory process and determine the forms of acute cholecystitis.Using color Doppler mapping in B-mode to visualize color loci in a longitudinal section of the gallbladder, we detected the presence of vessels in its wall, determined their localization and quantity. The cystic artery was depicted along the maximum possible length in the longitudinal section, which allowed us to correct the direction of flow using an angular mark and obtain the most accurate quantitative indicators of blood flow velocity (Figure 1).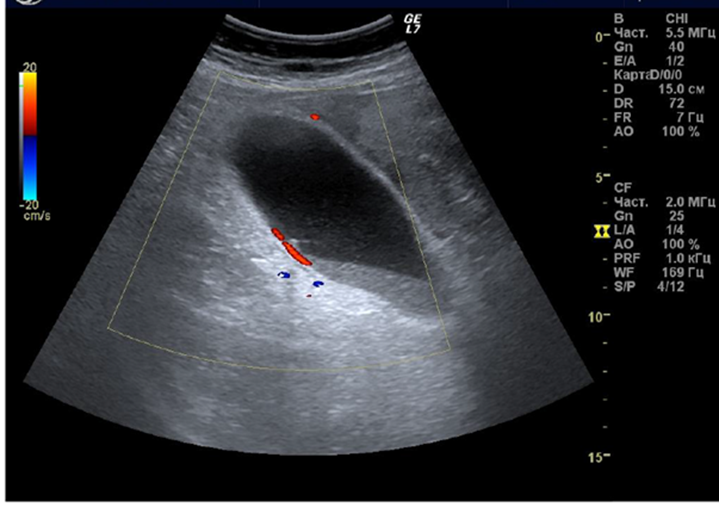 | Figure 1. Ultrasound duplex scanning of the gallbladder: in B-mode, its longitudinal section, the color locus from the artery is visualized in red |
Blood flow in the gallbladder wall was assessed according to the classification of Uggowitzer M. et al. (1997) and blood flow was defined as avascular, hypovascular, midvascular and hypervascular, which was respectively assessed as "0" degree, "+" degree, "++" degree and "+++" degree of wall vascularization. Standard quantitative indicators of blood flow velocity were studied, such as maximum systolic blood flow velocity (Vmax) and minimum systolic blood flow velocity (Vmin). The parameters of the Doppler device included a filter with a value of 100, a pulse repetition frequency in the range from 1.0 to 4.5 kHz and a control volume of 1 mm. (Figure 2)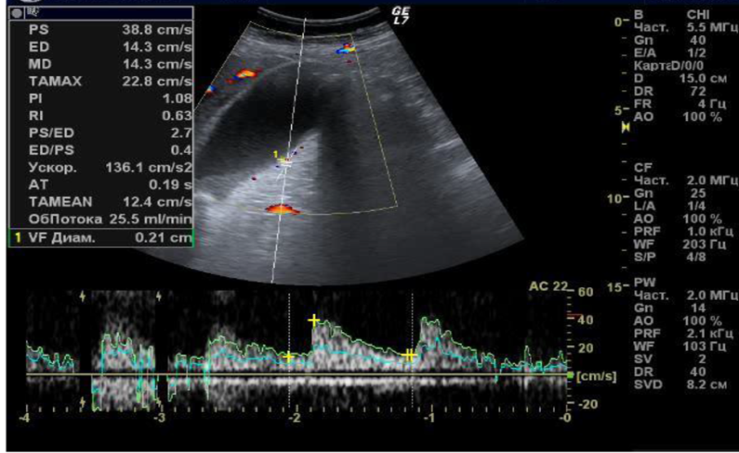 | Figure 2. Ultrasound color duplex scanning of blood flow a. cystica wall of the gallbladder. The spectrum corresponds to the arterial type of blood flow |
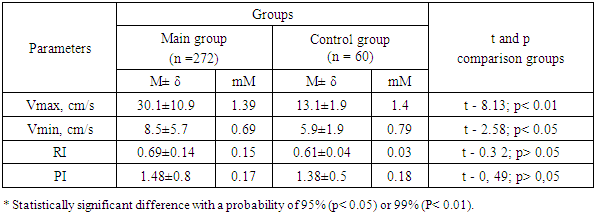
In the ultrasound duplex scanning of the gallbladder of 272 patients with acute hepatitis with comorbid cardiovascular diseases, in 208 (76.5%) cases, the gallbladder wall was visualized by arteries, and we assessed this as an arterial type of blood flow. In 64 (23.5%) cases, in addition to visualization of arteries, veins were also visualized, which we assessed as an arterial-venous type of blood flow.When analyzing the arterial blood flow in the gallbladder wall, an increase in the parameters Vmax and Vmin was revealed in the main group of patients, compared with the parameters of the control group in AC, the values of which statistically significantly differ with a probability of differences of 99% and 95% (p<0.01 and p<0.05). The data on arterial blood flow in the vessels of the gallbladder wall are presented in Table 2.Table 2. Parameters of arterial blood flow in the cystic artery in the wall of the gallbladder in patients with acute cholecystitis and comorbid cardiovascular diseases
 |
| |
|
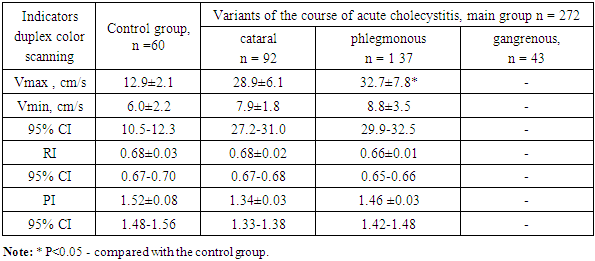
Analysis of the study data revealed a significant increase in the maximum blood flow velocity (Vmax) compared to the minimum velocity (Vmin). The Vmax values increased by 2.3 times, and Vmin - by 1.4 times. We assume that the increase in blood flow in the gallbladder wall in the color Doppler mode is associated with an increase in the number of vessels and expansion of their lumen in the phase of arterial hyperemia, which is characteristic of the infiltrative stage of the acute inflammatory process. This condition is usually defined as hypervascularization in the literature on ultrasound diagnostics [7,10]. However, when comparing the quantitative values of blood flow in the gallbladder wall in patients with acute cholecystitis and the control group, we found only a statistically significant increase in Vmax by 80% (p<0.05). Other blood flow parameters, such as Vmin, resistance index (RI) and pulse index (PI), tended to increase in values, but did not reach statistical significance compared to the values of healthy people. Our data from the study of patients with acute cholecystitis with comorbid cardiovascular diseases allow us to draw the following conclusions: the main Dopplerographic criterion of acute cholecystitis is an increase in the maximum systolic velocity (Vmax) of blood flow in the branches of the cystic artery of the gallbladder wall. The PI level in patients with acute cholecystitis was comparable with the parameters in the control group.In accordance with the rules of blood circulation, changes in blood flow in patients of the main group indicate low vascular tone of the microcirculatory bed of the gallbladder wall, as a result of increased arterial blood flow to the cystic artery, as a result of the development of the “arterial hyperemia” phase of the inflammatory process in the gallbladder.Thus, echographic studies using Dopplerography in AC and comorbid CVD, especially in complications, have prognostic value. The appearance of multiple vascular signals in a thickened and markedly heterogeneous wall of the gallbladder during Doppler examination indicates inflammatory changes, which are known to be pathomorphologically characterized by hypervascularization due to the reaction of the microvascular bed, which is typical for the infiltrative phase of inflammation. Uncomplicated AC was characterized by a marked increase in blood flow velocities (V max and V min) in the arterial system of the cystic duct, compared with the control comparison group.The study of the results of duplex scanning and determination of the blood flow velocity in the cystic artery, which were carried out with the aim of more accurately determining the diagnosis and the degree of inflammatory microcirculatory changes in the wall of the gallbladder, made it possible to determine the intensity of inflammation and morphological changes in the gallbladder, from the catarrhal form of inflammation to the gangrenous form, with the development of destruction of the gallbladder and the progression of peritonitis. Of the 272 patients examined, 92 were found to have catarrhal (33.8%), 137 had phlegmonous (50.4%), and 43 had gangrenous (15.8%) cholecystitis.The blood flow velocity in a. cystica and the peripheral resistance index - RI (Purcello index) were determined at three points of the gallbladder, as well as near the liver bed, with subsequent averaging of the parameters.Of the 43 patients with the gangrenous form, blood flow was not detectable in any patient. Blood flow velocity indices according to color duplex scanning of the a. cystica branches of the gallbladder wall depending on the forms of acute cholecystitis are presented in Table 3.Table 3. Blood flow velocity according to color duplex scanning of the branches of a. cystica of the gallbladder wall depending on the forms of OC
 |
| |
|
We found reliable significant differences in blood flow velocity in patients with phlegmonous inflammation of the gallbladder (32.8±7.6), compared with the parameters of the control group (P<0.05).It was determined that the visualization of blood flow in the wall of the a. cystica of the gallbladder mainly depended on its speed and the nature of inflammation. This means that the speed of arterial blood flow in the wall of the gallbladder indicates the degree of inflammatory reaction in patients with acute cholecystitis. According to our study, the values of the Gosling pulsatility index (PI) were reduced in all forms of acute cholecystitis. In individuals in the control group, the Gosling pulsatility index PI was the highest (1.52). PI was the lowest in patients with catarrhal cholecystitis and was not determined in patients with gangrenous inflammation (1.34 and 0), respectively. Purcell's index (RI) in the wall of the gallbladder was also, according to our study, a sensitive method for determining the degree of GB inflammation. RI was the lowest in patients with phlegmonous cholecystitis and was not determined due to the absence of blood flow in patients with gangrenous inflammation (0.65 and 0), respectively, without statistically significant differences. The absence of visualization in the gangrenous form is apparently associated with thrombosis of the gallbladder vessels, the lack of the ability to visualize hemodynamics in small vessels with a relatively low linear blood flow velocity in them.In order to dynamically monitor the activity of the inflammatory process, we conducted daily ultrasound examinations and color duplex scanning of the gallbladder vessels. We came to the conclusion that the most sensitive data were provided by the ultrasound color duplex scanning of the gallbladder vessels, which made it possible to actually determine the blood circulation in the gallbladder wall and, accordingly, to determine the degree of inflammation progression and the destructiveness of the process in the gallbladder wall.The algorithm we developed for selecting the tactics and timing of treatment of acute cholecystitis in patients with concomitant CVD is based on the data of ultrasound color duplex scanning and studying the state of blood flow in the gallbladder wall, determining its disturbance and identifying, respectively, sclerosis or thrombosis of arterial vessels (branches of a. cystica), which can serve as the basis for the rapid development and progression of destruction of the gallbladder wall, with the development of peritonitis. This diagnostic procedure made it possible in all cases to determine the morphological form of development of acute cholecystitis and identify complications. Such a comprehensive approach to determining the morphological forms of the course of acute cholecystitis significantly increased our capabilities for early diagnosis and choosing the correct tactics for treating patients with acute cholecystitis and concomitant complications.We took as a basis that patients with catarrhal cholecystitis and comorbid cardiovascular diseases, in the absence of data for destructive changes in the gallbladder do not need emergency surgical interventions. This category of patients has indications for surgical interventions, but they can be postponed or canceled due to the severity of the comorbid cardiovascular disease. Thus, the possibility of drug therapy of general somatic pathology is created. In cases of acute phlegmonous cholecystitis, there is no doubt that an urgent surgical intervention is needed for vital indications, although the patient has severe comorbid cardiovascular diseases. In this situation, we consider the issue of using minimally invasive interventions to decompress the gallbladder and bile ducts, followed by radical surgery. In patients with a gangrenous form of acute cholecystitis, we performed emergency surgery.
4. Conclusions
The main criterion of ultrasound color duplex scanning of acute cholecystitis is an increase in the maximum systolic velocity (Vmax) of blood flow in the branches of the cystic artery in the wall of the gallbladder.The results of our study indicate that the use of ultrasound color duplex scanning as a non-invasive method allows us to determine the morphological form of acute cholecystitis and the presence of a destructive process in the gallbladder, which is important when making informed decisions about the need for surgical intervention.Ultrasound color duplex scanning of acute cholecystitis is an opportunity to determine the degree of risk of surgical intervention depending on the volume of surgical intervention performed.
References
| [1] | Abdurakhmanov M.S. Ruziev U.U. Issues of complex treatment of acute cholecystitis in patients with decompensated pathology of the cardiovascular system “Journal of Theoretical and Clinical Medicine”, No. 4, 2020, pp. 35-41. |
| [2] | Verzakova I.V., Timerbulatov M.V., Usatova O.S., Makaryeva M.L. Hemodynamics based on duplex scanning in the visceral branches of the abdominal aorta in acute calculous cholecystitis complicated by mechanical jaundice // Medical Bulletin of Bashkortostan. 2006. No. 1. P. 27-28. |
| [3] | Karimov Sh.I., Kim B.J.I., Khakimov M.Sh. Choice of surgical treatment of acute cholecystitis in patients with increased surgical risk // Annals of surgical hepatology. 2004. Vol. 9, No. 1. P. 115–119. |
| [4] | Kulikov V.P. Fundamentals of ultrasound examination of vessels M.: Publishing house Vidar-M, 2015. 392 p. |
| [5] | Mitkov V.V. Dopplerography in diagnostics of diseases of the liver, gall bladder, pancreas and their vessels. Moscow: Publishing house Vidar-M, 2000. 152 p. |
| [6] | Mitkov V.V., Mitkova M.D., Mumladze R.B. Possibilities of Doppler research methods in diagnostics of inflammatory diseases of the gallbladder // Ultrasound diagnostics. 2000. No. 1. P. 5-14. |
| [7] | Regional hemodynamics in chronic cholecystitis and gallbladder conditions without chronic inflammation based on color duplex scanning / O.V. Verzakova, I.V. Verzakova // Medical Bulletin of Bashkortostan. - 2017. Vol. 12. - No. 1 (67). - P. 32-36. |
| [8] | Abelson JS, Afaneh C., Rich BS, Dakin G., Zarnegar R., Fahey TJ Advanced laparoscopic fellowship training decreases conversion rates during laparoscopic cholecystectomy for acute biliary diseases: a retrospective cohort study // Int. J. Surg. 2015. 13. P. 221-226. |
| [9] | Borzellino G., Motton AM, Minniti F., Tomezzoli A. Sonographic diagnosis of acute cholecystitis in patient with symptomatic qallstones // J. Clin. Ultrasound. 2015. 24. P. 10. |
| [10] | Jeffrey RB, Nino-Murcia M, Ralls PW et al. Color Doppler sonography of the cystic artery: comparison of normal controls and patients with acute cholecystitis. J. Ultrasound Med., 1995, Vol. 14, pp. 33-36. |
| [11] | Lee HJ, Choi BI, Han JK et al. Three-dimensional ultrasonog raphy using the minimum transparent mode in obstructive biliary diseases: early experience. J. Ultrasound Med., 2002, Vol. 21, No. 4, pp. 443-453. |
| [12] | Paulson EK, Kliewer MA, Hertzberg BS Diagnosis of cholecystitis with color Doppler sonography: significance of arterial flow in thickened gallbladder wall. AJR., 1994, Vol. 162, pp. 1105-1108. |
| [13] | Schiller VL., Turner RR, Sarti DA Color Doppler imaging of the gallbladder wall in acute cholecystitis: sonographic-patho-logic cor relation. Abdom. Imaging, 1996, Vol. 21. P. 233-237. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML