-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(10): 2683-2687
doi:10.5923/j.ajmms.20241410.49
Received: Sep. 1, 2024; Accepted: Sep. 29, 2024; Published: Oct. 30, 2024

Improving Treatment and Rehabilitation of Children with Hearing Loss Due to Toxoplasmosis and Cytomegalovirus Infection
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKarimova Munisa Mansurovna1, Amonov Shavkat Ergashevich2, Nasiba Rakhimovna Jabbarova3
1PhD Student of the Department of Otorhinolaryngology No.2, Samarkand State Medical University, Uzbekistan
2Doctor of Medical Sciences, Professor, Head of the Department, Department of Otorhinolaryngology, Pediatric Otorhinolaryngology and Pediatric Dentistry, Tashkent Pediatric Medical Institute, Uzbekistan
3Assistant of Clinical and Laboratory Diagnostics, Department of Samarkand State Medical University, Samarkand State Medical University, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Treatment of sensorineural hearing loss (SNHL) over the last decades remains one of the most urgent problems of modern otorhinolaryngology and serology. Despite certain successes achieved in recent years, the number of people with hearing defects is increasing to a large extent due to this pathology. According to some authors, SNHL on the background of toxoplasma and CMV infection significantly affects the quality of life of children, in addition, the importance of the issues of diagnosis, treatment and rehabilitation of patients with hearing loss is largely determined by the fact that this pathology is among the socially significant and affects all age groups of the pediatric population. Despite the availability of a variety of methods for the treatment of SNHL on the background of toxoplasma and CMV infection, the problem is far from being solved. Drug therapy of sensorineural hearing loss based on the etiological factor and background diseases leads to increased treatment efficacy and improved socialization of children. Therefore, an urgent and reasonable task in the problem of treatment of SNHL is the search for new methods of therapy depending on the etiologic factor of this pathology.
Keywords: Cytomegalovirus infection, Toxoplasma infection, Interleukins, Sensorineural hearing loss, Luciferin
Cite this paper: Karimova Munisa Mansurovna, Amonov Shavkat Ergashevich, Nasiba Rakhimovna Jabbarova, Improving Treatment and Rehabilitation of Children with Hearing Loss Due to Toxoplasmosis and Cytomegalovirus Infection, American Journal of Medicine and Medical Sciences, Vol. 14 No. 10, 2024, pp. 2683-2687. doi: 10.5923/j.ajmms.20241410.49.
1. Introduction
- Despite the achievements in the field of otorhinolaryngology to this day sensorineural hearing loss is one of the leading places in the structure of pediatric morbidity. According to WHO data, the incidence of hearing loss in children ranges from 1 to 2% and 0.02% of them are children with sensorineural hearing loss of various degrees. It has been revealed that in early childhood this type of hearing loss occurs in 82% of children, i.e. before the development of speech, it should be noted that, of these children, in the perinatal period, disorders appear in 38.5% of children.Analysis of foreign and domestic literature has shown that the pathogenesis of hearing loss in children and adults is based on multifactorial causes. Over the last 15 years, the incidence of sensorineural hearing loss in Uzbekistan, especially in young children, has more than doubled. Currently, almost 7% of the population has hearing impairment, with sensorineural disorders accounting for 70-80%. In recent decades, there has been a trend towards an increase in the incidence of SNHL hearing loss in children, with viral infections being the main cause. Analysis of the literature has shown that researchers have studied the clinical and audiological characteristics of sensorineural hearing loss (SNHL) due to the association of toxoplasma and CMV infection. The aim of the study is to improve the results of treatment and rehabilitation in children with hearing loss on the background of toxoplasma and cytomegalovirus infection and on this basis to develop a therapeutic and diagnostic algorithm.
2. Materials and Methods
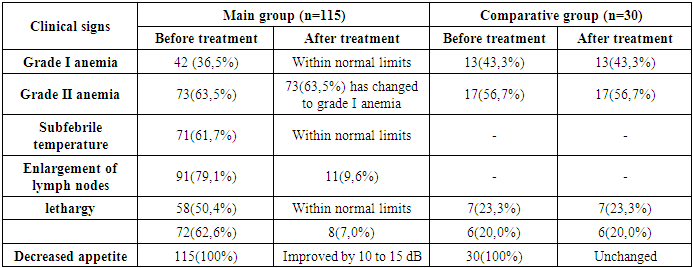
- The work was carried out in the period from 2021 to 2023 at the Department of Otorhinolaryngology №2 and in the Consultative Polyclinic of the Multidisciplinary Clinic of Samarkand State Medical University. The object of the study was 115 children in the age category from 1 to 7 years with SNHL in association with toxoplasmosis and CMV, who were included in the main group and in the comparison group of 30 children diagnosed with SNHL without toxoplasmosis and CMV infection. Group I patients received traditional therapy according to the age dosage, in combination of antiviral (Proteflazid) and immunocorrective therapy (Galavit 50 mg in the form of suppositories according to the scheme). Group II patients received only conventional therapy. The diagnosis of sensorineural hearing loss was formed (H90.3 Bilateral sensorineural hearing loss) according to WHO requirements and classified according to the international classification of disease ICD-10. Anamnestic, clinical, laboratory, and instrumental examination data of patients were taken into account in making the diagnosis of the disease. All patients were examined by general clinical, clinical-immunologic, and virologic methods. Infection with toxoplasmosis and CMVI pathogens was determined by enzyme-linked immunosorbent assay (ELISA) and polymerase chain reaction (PCR). Endoscopic ear examination, tympanometry, OAE and SHLHP were also performed in all patients. The results of the study of anamnestic data on the causes of hearing loss revealed that the main cause of hearing loss in sick children was an unfavorable course of pregnancy in mothers against the background of toxoplasma and cytomegalovirus infection. In the course of objective examination the following clinical signs were found in the patients: in the main group all 115 (100%) patients showed signs of anemia, in the comparative group this index was 43.4% (13) respectively, sub febrile temperature in the main group was observed in 61.7% (71) patients, enlarged lymph nodes in the main group were palpated in 91 (79.1%) patients, 50.4% (58) cases were observed lethargy in children of the main group, decreased appetite in both groups was found in 72 (62.6%) and 6 (20%) patients respectively. No enlargement of lymph nodes, sub febrile temperature and lethargy was observed in children in the comparison group in 7 (23.3%) children respectively.The results obtained on CSVC showed that in the main group I degree of SNHL was registered in 17 (14.8%) patients, in the comparison group in 4 (13.3%) children. II degree of SNHL in 35 (30.4%) in the main group, 10 (33.3%) in children of the comparison group. In 53 (46.1%) children of the main group and in 8 (26.7%) children of the comparison group the III degree of SNHL was registered. IV degree of SNHL was registered in 10 (8.7%) children of the main group and in 8 (26.7%) children of the comparison group. The results of our research showed that in all the studied children in both groups tympanometry revealed type A and the result of OAE was evaluated as "failed".To confirm the presence of these infections, we performed molecular diagnostics (PCR). In children of the main group DNA of toxoplasma and CMV infection was detected in blood serum and in the comparison group PCR result was negative. The results of immunologic examination of children, showed that the characteristic signs before treatment in the main group were found to be increased content of proinflammatory interleukins IL-4, IL-18, as well as lactoferrin, total and high-sensitivity C-reactive protein (table 1).
|

|
3. Results and Discussions
- After treatment specific antibodies IgM to toxoplasmosis and CMV in the main group significantly decreased to the level of normal 0,26±0,01 and 0,52±0,01 respectively, which shows the cure of acute period of infection (p<0,001). Specific IgG antibodies to toxoplasmosis and CMV in this group after treatment significantly amounted to 0.25±0.00 and 0, 048±0.02 respectively, which indicate the beginning of remission (p<0.001). It should be noted that in the comparative group after the treatment there were no tests for specific antibodies to toxoplasmosis and CMV infection, as this group consisted of patients with SNHL without these infections.In order to solve the set objectives, we also performed post-treatment SHLHP in the studied groups. As the results showed, in group I children with SNHL on the right side was diagnosed in 38.31±1.12 patients, SNHL on the left side in 47.31±1.12 patients. As for the comparative group with SNHL I degree on the right side, it was significantly diagnosed in 28.0±2.83 patients (p<0.001). On the left side, this degree in the comparison group was diagnosed in 37.5±3.54 patients, respectively (p<0.001). SNHL of I-II degree on the right side in the main group was diagnosed in 48,81±0,07 patients, on the left side in 58,3±0,96 patients. The distinctive feature of this index was that in the comparison group, in 39.0±1.12 patients, I-II degree SNHL of the right side was reliably determined in 39.0±1.12 patients (p<0.001), while on the left side it was reliably determined in 50.0±2.50 children (p<0.01). Grade II SNHL on the right side in the main group was determined in 56.52±0.75 children and on the left side in 62.61±0.63 children (p<0.001).In the comparison group, this degree of SNHL on the right side was significantly diagnosed in 46.25±2.02 children and on the left side in 51.00±2.26 patients, respectively (p<0.001). There was not a strong feature of difference between the main and comparison group in the occurrence of SNHL grade II-III on the right side, which was reliably diagnosed in 62.63±0.82 of the main group and 52.50±1.87 patients of the comparison group respectively and on the left side in 65.53±0.54 and 60.83±0.91 patients respectively by group (p<0.001). In the comparative aspect, in the main group children, SNHL of grade III was diagnosed on the right in 65.45±0.32 and on the left in 72.91±0.54 patients, in the comparison group on the right in 61.25±1.44 and on the left in 68.75±1.44 patients respectively (p<0.01). Prominent improvements in the main group of SNHL grade III-IV on the right side was diagnosed in 76.57±1.00 children and on the left side in 96.29±0.70 children respectively (p<0.05). The main tendencies in hearing improvement were observed in the main group, which received complex therapy, as the IV degree SNHL on the right side was diagnosed in 94.00±1.41 children (p<0.001) and on the left side in 96.00±1.41 children, respectively (p<0.01). It should be noted that children in the comparison group did not show positive hearing dynamics after the traditional treatment, the results of CSVI remained unchanged. The given results of clinical observation testify to a reliable improvement of hearing in children of the main group who received complex treatment, which in total showed normalization of hearing on the right in 19.13±1.04 and on the left in 23.50±0.70 cases (p<0.001) (table 3).
 | Table 3. The results of the correlation of the obtained results of SHLHP after treatment in children of the main and comparison groups |
 | Table 4. Correlation analysis between specific antibodies and immune status after treatment |
4. Conclusions
- Those, our studies have shown strong correlations between specific antibodies of pathogens, cytokine status, and inflammatory proteins. The obtained data can be used as therapeutic criteria for SNHL in the association of toxoplasma and CMV infection. Changes in immunological parameters imply the inclusion of antiviral, antioxidant and immune-correcting drugs, the use of which improve clinical signs and laboratory parameters.