-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(10): 2616-2623
doi:10.5923/j.ajmms.20241410.36
Received: Sep. 13, 2024; Accepted: Oct. 10, 2024; Published: Oct. 24, 2024

Outcomes of Application of a Complex Postload Recovery Program by Paralympic Judokas
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSattarova Diana Bakhtiyarovna1, Usmankhodjaeva Adibaxon Amirsaidovna2
1Doctor of the Department of Rehabilitation, Traditional Medicine and Physical Culture “Tashkent Medical Academy”, Republic of Uzbekistan
2Doctor of Medical Sciences, Head of the Department of Rehabilitation, Traditional Medicine and Physical Culture at the Tashkent Medical Academy, Republic of Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The objective of the study is to assess the effectiveness of the improved post-load recovery program in athletes of the Paralympic National Judo Team of the Republic of Uzbekistan. Materials and methods. The clinical pilot study recruited all visually impaired athletes (54 judoists) of the Paralympic team of Uzbekistan who were randomly allocated into 2 groups: study and control group to perform two post-load recovery programs: standard and improved. The comprehensive improved program included individual assessment of physical, psycho-emotional, and social health parameters during the training and recovery stages, before a tournament and after the completion of the post-load recovery program. Results. Before studying application of the Advanced Post-Load Recovery Program a number of shortcomings in the existing Post-Load Recovery program were revealed. The outcomes of the study enabled to find out a statistically significant difference between the indicators of load tests in Paralympic judoists after the end of the recovery period. At the same time, the best indicators of anaerobic and aerobic indicators of physical performance were recorded in the group of study participants practicing the improved post-load recovery program. In addition, a shorter period of energy recovery was noted, including muscle activity. Conclusions. The findings obtained during the pilot study indicate the advantages of the comprehensive improved post-load recovery program used by Paralympic judoists taking into account their physical, psychological, and social health parameters. This observation is extremely important, as the reorganization of the recovery period of athletes after the competition can contribute to improved aerobic potential, increased anaerobic power indicators, as well as effective management of energy resources during periods of intense physical activity.
Keywords: Visually impaired Paralympians, Load Testing, Physical recovery programs
Cite this paper: Sattarova Diana Bakhtiyarovna, Usmankhodjaeva Adibaxon Amirsaidovna, Outcomes of Application of a Complex Postload Recovery Program by Paralympic Judokas, American Journal of Medicine and Medical Sciences, Vol. 14 No. 10, 2024, pp. 2616-2623. doi: 10.5923/j.ajmms.20241410.36.
Article Outline
1. Introduction
- The development of sports in Uzbekistan is one of the priorities of the government. A number of new government documents provide for the need to modernize and optimize programs for medical and biological support of sports and training of athletes. The victories of Uzbek athletes at world-class competitions arouse interest and attention to the country’s sports community as a whole. Paralympic sport is no exception, and Paralympic athletes of Uzbekistan successfully perform in prestigious world arenas. Judo is one of the priority sports areas in the Republic of Uzbekistan. Paralympic athletes who are part of the national team have high results according to the ratings of the International Blind Sports Federation [1]. To achieve high professional results, Paralympic judokas systematically need to improve their individual physical and functional performance [2]. Extreme intensity of a judoka’s work in preparation for international competitions and the Paralympic Games requires careful medical health monitoring of para-athletes and requires the use of effective physical recovery programs [3]. The main objective of post-exertional recovery programs is to create the most effective way for a para-athlete to recover from the state of metabolic and energy imbalance associated with physical activity [4]. In addition to compensatory effects on the physical and functional health parameters of para-athletes, post-load recovery programs help maintain a satisfactory level of psycho-emotional state parameters caused by stress in response to excess load [5]. Based on modern scientific research in the field of sports medicine, there is a particular interest and emphasis on studying the relationship between load testing indicators at different stages of high-class athletes' professional careers [6]. Despite this, standardized protocols for post-exercise recovery programs have not yet been developed for professional judokas who are part of national Paralympic teams [7]. It is worth noting that the complexity of developing such programs is related to the multifaceted impact of extreme load levels on athletes' health parameters. Post-exercise recovery programs can serve as a tool for reducing the risk of injury, correcting physical and psychosocial health parameters, and significantly influencing an athlete's long-term professional success [8]. The advantage of implementing optimized post-exercise recovery programs is the improvement of individual physical fitness levels, allowing athletes to have better physical and functional indicators before the start of competitions [9]. Additionally, post-exercise recovery programs help athletes cope with the emotional and psychological stress associated with the high physical load during competitions [10]. Personalized physical recovery programs include measures aimed at improving all health parameters, such as regulating sleep and nutrition, physical rehabilitation, psychotherapy, and individualizing the training regimen [11,12]. Therefore, studying the impact of professional activities on the physical and functional health parameters of judokas is a crucial task. Solving this will allow for the creation of the most suitable post-exercise recovery program and the reorganization and improvement of the professional training processes for Paralympians [13].Objective of the Study: To assess the impact of an improved protocol in a personalized post-exercise recovery program on the physical and functional parameters of Paralympic judokas.
2. Materials and Methods
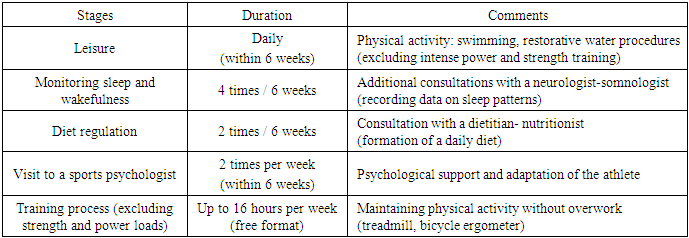
- A pilot clinical study involved 54 visually impaired professional judokas who are part of the national Paralympic team of the Republic of Uzbekistan. The study design adhered to the international protocol for experimental clinical trials "CONSORT 2010," by L. Thabane et al. (2016) [14], (Fig. 1). The athletes were randomly assigned to two groups using a computer program (Statistical methods: Randomization and random sampling procedures) following a fixed randomization principle, 1:1. The observation period for the athletes was 12±1.5 months, including the preparation period for international competitions, the competition period itself, and the physical recovery period after the competitions. The average age of the Paralympians was 24±3.1 years, with an age median ranging from 19 to 32 years. The weight category of the judokas and the class of visual impairment among the study participants were stratified using the International Blind Sports Federation (IBSA) classifier. According to IBSA classification: B1: visual acuity worse than 2.60 according to the logarithm of the minimum angle of resolution (LogMAR); B2: visual acuity ranges from 1.50 to 2.60 on LogMAR and/or a visual field narrowed to a diameter of less than 10°; B3: visual acuity from 1 to 1.40 on LogMAR and/or a visual field narrowed to a diameter of less than 40°. The Paralympians were divided into two groups depending on the type of post-exercise recovery program (PRP) after preparation and participation in major international competitions. It is worth noting that the study participants had between 1 and 4 matches during the competition period. Group I, consisting of 27 (50.0%) judokas, included athletes who followed a standard post-exercise recovery program (SPRP) after a 46-week preparation period for the competition. Group II consisted of 27 (50.0%) judokas who participated in an improved post-exercise recovery program after a 46-week preparation period for the competition. The improved post-exercise recovery protocol (IPRP) included 6 weeks of active rest, with coordination of sleep and wakefulness patterns under the regular supervision of the team’s sports physician, sports psychologist, and nutritionist. The program included systematic visits to a clinical sports psychologist (twice a week for 1.5 months), 16 hours of training per week in a free format, excluding excessive strength and power loads (Table 1).
|
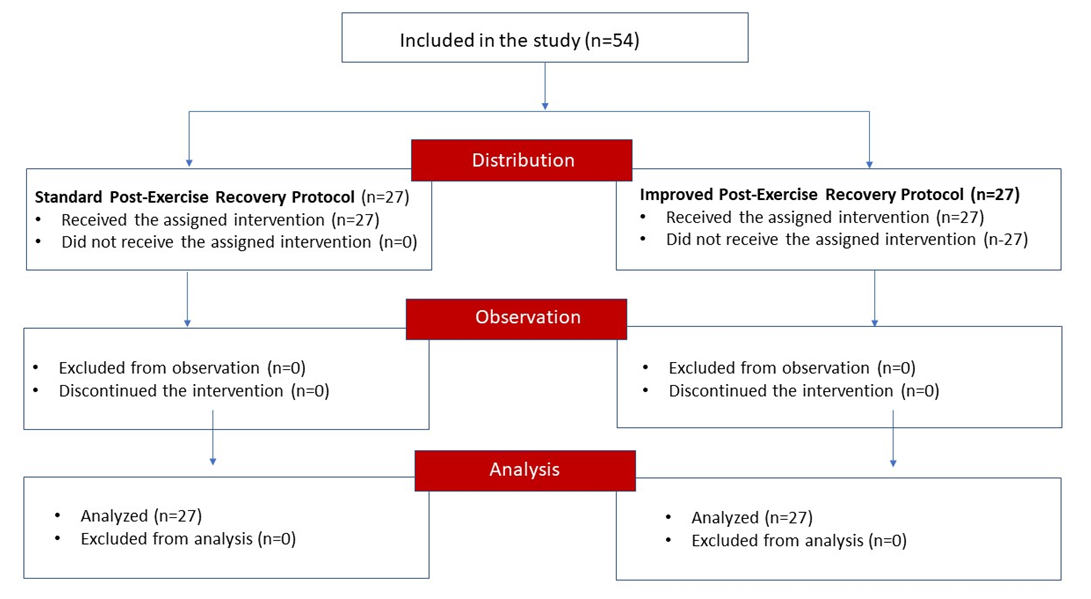 | Figure 1. Flow-diagram of pilot trial in CONSORT format |
3. Results
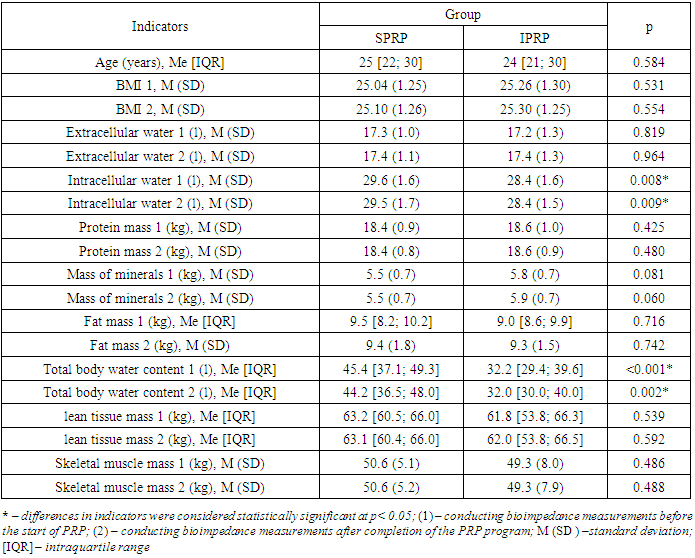
- The study revealed that the morphometric indicators obtained through bioimpedance analysis did not show significant differences between the study participants based on their group assignment. The exceptions were the indicators of intracellular water content and total body water content in the Paralympians, which demonstrated statistically significant differences (p<0.05), (Table 2).
|
|
|
|
|
|
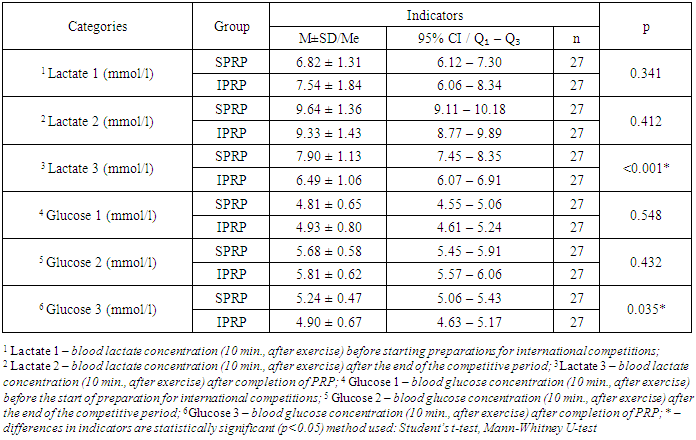
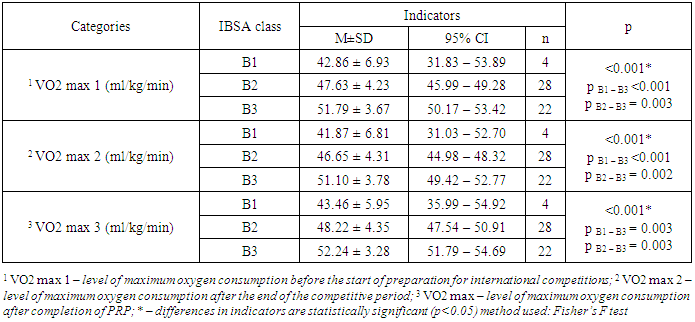
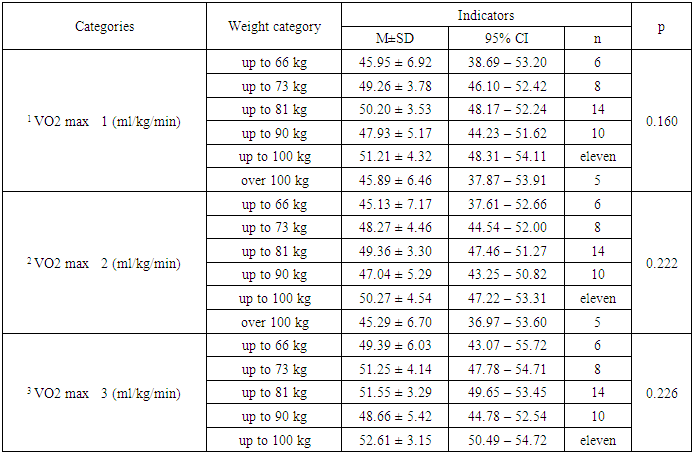
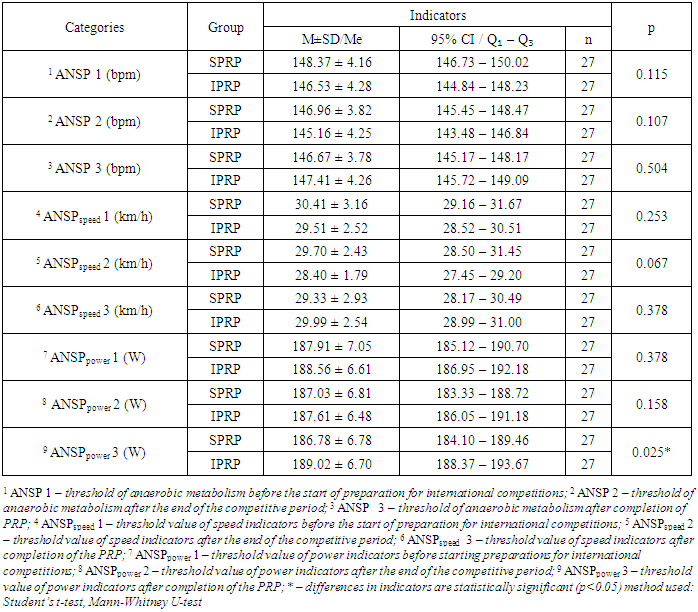
4. Discussion
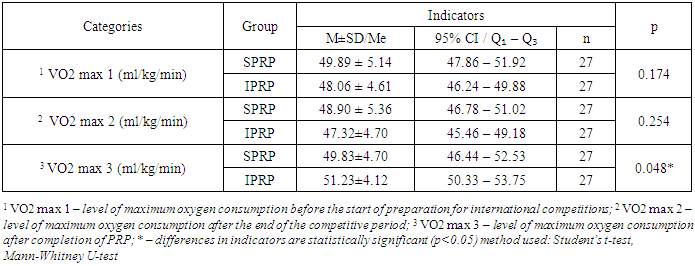
- The developed comprehensive post-exercise recovery program for judo athletes was based on the need to analyze the physical, mental, and social health parameters of Paralympians as a whole. This pilot project emphasizes the need for an individualized approach to athlete preparation and recovery. Normalizing periods of active rest, sleep, nutrition, and the athlete's psycho-emotional state, which are often overlooked by coaches, plays a crucial role. The application of the improved and personalized recovery program within this clinical study revealed improvements in various indicators of physical and functional status among judokas. Notably, an increase in VO2 max by 4.0% was recorded, indicating a higher aerobic capacity among participants following the IPRP compared to those following the standard program (p=0.048). The optimized recovery program, based on the data showing better VO2 max indicators, may positively impact endurance and overall athletic performance in judokas. Additionally, significant differences in VO2 max were observed depending on the class of visual impairment according to IBSA, confirming the previously hypothesized link between the severity of visual impairment and the physical and functional parameters of professional parasport athletes. Furthermore, among participants who received the IPRP, a significant 2.0% increase in power output (ANSPpower) was observed compared to the standard program group (p=0.025). This may indicate a more effective use of anaerobic energy production mechanisms, which is particularly important for judokas requiring short-term, intense efforts during matches. Metabolic compensation also proved to be higher in the experimental group of athletes who received the IPRP. Analysis of lactate and glucose levels in capillary blood showed that participants using the IPRP had a higher level of recovery capacity for energy deficits related to peak physical load thresholds. Additionally, the analysis of lactate and glucose concentrations confirmed more effective management of energy resources in athletes from the experimental group.
5. Conclusions
- Overall, the results of this study highlight the advantages of using the improved IPRP protocol among Paralympic judokas, particularly in terms of aerobic capacity, anaerobic power output, and energy resources during intense physical exertion. The results of the exercise testing in response to the IPRP represent a significant achievement and could potentially contribute to the reorganization of recovery approaches for athletes post-competition. This could greatly enhance athlete performance in competitions, improve recovery between training sessions, and reduce injury risk. Based on the obtained data, the research team recommends further investigation of the IPRP protocol within a larger clinical study. Future research could be a crucial step toward developing optimal physical training programs to achieve high sporting results and maintain satisfactory performance levels among Paralympians.Study Limitations. The limitations of this study are related to the small sample size, and the limited number of participants is due to the restricted number of individuals on the Uzbekistan Paralympic judo team. Future research on rehabilitation and post-exercise recovery programs should take this factor into account.Conflict of Interest and Funding: The authors of the study declare no financial or other conflicts of interest.
Authors' Contributions
- 1. Diana Bakhtiyarovna Sattarova contributed to the choice of study design, data collection and data analysis;2. Usmankhodjaeva Adibakhon Amirsaidovna contributed to the critical revision of the article and final approval of the version of the article for publication.
ACKNOWLEDGEMENTS
- The authors express gratitude to the leadership of the Republican Scientific and Practical Center for Sports Medicine represented by its director Sirozhiddinov K.K. in providing assistance in conducting research and collecting material.