-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(10): 2514-2517
doi:10.5923/j.ajmms.20241410.14
Received: Sep. 18, 2024; Accepted: Oct. 12, 2024; Published: Oct. 17, 2024

Assessment of Quality of Life Indicators of Patients with Cirrhosis of the Liver
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLOtajonov I. O.1, Urinov A. M.2
1Tashkent Medical Academy, Uzbekistan
2Alfraganus University, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

In order to assess the social environment, disease status, and quality of life indicators of patients with cirrhosis of the liver, an SF-36 survey proposed by the World Health Organization was used to determine the quality of life of 89 patients. The results obtained indicate a reliable difference in all scales of the SF-36 survey among individuals with liver cirrhosis and healthy. Thus, the quality of life data contribute to the individualization of the treatment program, determine its effectiveness and prognosis. To objectify the quality of life indicator, the testological approach has become widespread.
Keywords: Cirrhosis of the liver, An indicator of quality of life, Indicator, Testological approach
Cite this paper: Otajonov I. O., Urinov A. M., Assessment of Quality of Life Indicators of Patients with Cirrhosis of the Liver, American Journal of Medicine and Medical Sciences, Vol. 14 No. 10, 2024, pp. 2514-2517. doi: 10.5923/j.ajmms.20241410.14.
Article Outline
1. Introduction
- Quality of life is a construct that reflects the positive and negative aspects of an individual’s life. This construct is expanded upon by health-related quality of life (HRQL), which includes health risks and conditions, functional status, social support, and socioeconomic status on individuals’ well-being. Cirrhosis is the culmination of various pathways that can lead to the development of advanced hepatic fibrosis. These mechanisms include alcohol abuse, iron or copper overload, autoimmune liver diseases, biliary atresia, cystic fibrosis, and non-alcoholic fatty liver disease as well as chronic hepatitis B, chronic hepatitis C, and inborn errors of metabolism [1]. The most prevalent disease processes likely to result in cirrhosis in the United States include chronic hepatitis C virus (HCV), non-alcoholic fatty liver disease (NAFLD), and alcoholic liver disease (ALD) [2].Thus, the quality of life data contribute to the individualization of the treatment program, determine its effectiveness and prognosis. To objectify the quality of life indicator, the testological approach has become widespread. The use of specially developed questionnaires allows patients to be drawn to the joint determination of treatment tactics with the doctor and creates favorable conditions for successful therapy. [3]. Among the general methods for assessing quality of life, the SF-36 Health Status Survey questionnaire proposed by the Boston Institute of Health (J. Ware) has gained wide acceptance and is the main one in the International Project for Assessing Quality of Life [4,5].Purpose of the study: Assessment of the social environment, disease status and quality of life indicators of patients with cirrhosis of the liver.
2. Material and Methods
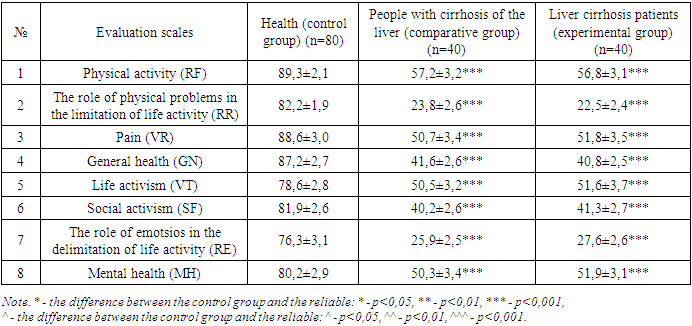
- From the medical cards of 89 patients treated in hospitals for the analysis of side diseases in patients (№025/U scale.) in his study of data on Anamnesis, attention was paid to the diseases he experienced, chronic diseases and foci of infectious diseases. Analysis of the disease was carried out according to the International Classification of diseases 10th revision, dividing them into classes and nasological forms.One of the statistical methods of modern medicine in determining the social hygienic description of patients, risk factors and quality of life of the disease was the use of the phenomenon-control research method. In this case, data was collected using a questionnaire from 30 people of the same age living in Tashkent in a control group to compare the data of patients in the main group. Of the patients in the control group, 43 were female and 46 were male. The SF-36 survey proposed by the World Health Organization was used to determine the quality of life of those involved in the study. It is considered general and helps to assess the quality of life of patients with various diseases and compare these indicators with a healthy population. In addition SF-36 is compiled for adults, covering respondents aged 14 years or older. It is characterized by a high efficiency of the questionnaire, short length (consisting of 36 questions), ease of application.It is characterized by a high efficiency of the questionnaire, short length (consisting of 36 questions), ease of application.Quality of life assessment criteria under SF-36 survey:1. Physical activity (RF)2. The role of physical problems in the limitation of life activity (RR)3. Pain (VR)4. General health (GN)5. Life activism (VT)6. Social activism (SF)7. The role of emotsios in the delimitation of life activity (RE)8. Mental health (MH) In the studied groups, Z-values were calculated on 8 indicators based on the formulas presented below, and the physical component of Health and mental components of Health were calculated.Calculation of the Z-value on scales.PF-Z = (PF – 84,52404) / 22,89490RP-Z = (RP – 81,19907) /33,797290BP-Z = (BP – 75,49196) /23,558790GH-Z = (GH – 72,21316) /20,16964VT-Z = (VT – 61,05453) /20,86942SF-Z = (SF – 83,59753) /22,37642RE-Z = (RE – 81,29467) / 33,02717MH-Z = (MH – 74,84212) / 18,01189.Calculation of physical components of Health.MHsum = (PF-Z* -0,22999) + (RP-Z* -0,12329) + (BP-Z* -0,09731) + (SF* 0,26876) + (MH-Z* 0,48581) + (RE-Z* 0,43407) + (VT-Z* 0,23534) + (GH-Z* -0,01571)MH = (MHsum* 10) + 50Calculation of mental components of Health.MHsum = (PF-Z* -0,22999) + (RP-Z* -0,12329) + (BP-Z* -0,09731) + (SF* 0,26876) + (MH-Z* 0,48581) + (RE-Z* 0,43407) + (VT-Z* 0,23534) + (GH-Z* -0,01571)MH = (MHsum* 10) + 50The data obtained was processed statistically, calculating the mean values (M), the standard deviation (σ) and the standard errors of the average value (m). To tolerate the reliability of the difference between the results, the Stoudent –t criterion and χ2 criteria were used. The difference between the indicators was assessed as reliable at P<0.05.
3. The Results Obtained and Their Discussion
- Together with the hepatoprotector, a survey of SF-36 was carried out in all respondents before the appointment of a pahrez table as well as a probiotic. The results obtained show that there is a reliable difference between individuals with cirrhosis of the liver and healthy in all scales of the SF-36 survey.
|
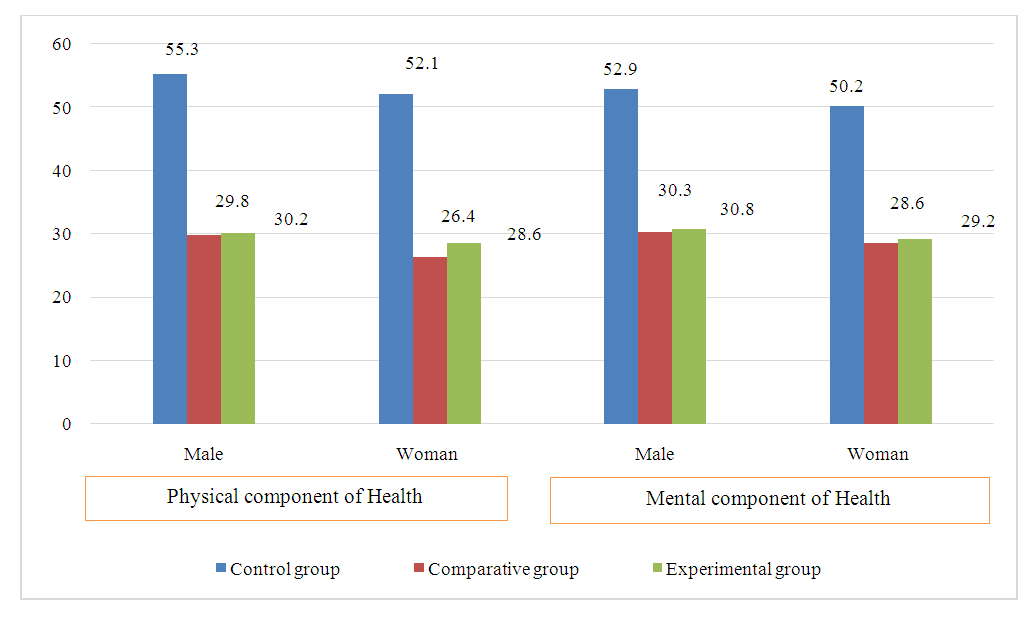 | Figure 1. Gender-based health components of groups |
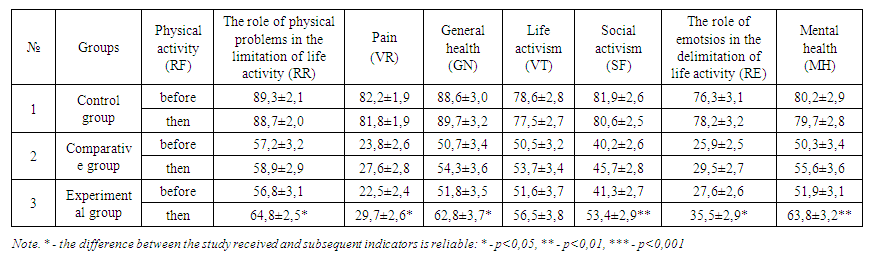 | Table 2. Pre-and post-research results on the criteria of the SF-36 survey |
4. Conclusions
- Patients with cirrhosis of the liver were also found to have a strong negative mean correlation (R=0.49). Patients were found to have a moderately strong inverse correlation relationship between the duration of the disease and the physical and mental components of Health (r=0.62 and R=0.58, respectively). It has been found that the correlation relationship between disease rates and the physical and mental components of Health is r=-0.65 and R=-0.61, respectively.