-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(9): 2295-2298
doi:10.5923/j.ajmms.20241409.36
Received: Aug. 27, 2024; Accepted: Sep. 15, 2024; Published: Sep. 20, 2024

The Effectiveness of Empagliflozin Depending on Body Mass Index in Patients with Chronic Heart Failure in the Vulnerable Phase
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhalikova A. O., Abdullev T. A., Tsoy I. A., Kurbanova D. Sh.
Republican Specialized Scientific-Practical Medical Center of Cardiology, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article given the high risk of an undesirable outcome, the first 3 months after discharge from the hospital in patients diagnosed with heart failure are usually defined as a vulnerable period or vulnerable phase. This period begins with discharge after acute heart failure and lasts up to 3 months after discharge. The vulnerable period can be divided into three phases: the very early phase (the first month after discharge), the early phase (up to 60 days after discharge) and the late phase (60-90 days after discharge). Due to the risk of early readmission and poor prognosis, the vulnerable period represents a window of opportunity to identify the phenotypes of patients at risk and interventions that can improve the prognosis.
Keywords: Risk and interventions, High risk, Hospital, Vulnerable period
Cite this paper: Khalikova A. O., Abdullev T. A., Tsoy I. A., Kurbanova D. Sh., The Effectiveness of Empagliflozin Depending on Body Mass Index in Patients with Chronic Heart Failure in the Vulnerable Phase, American Journal of Medicine and Medical Sciences, Vol. 14 No. 9, 2024, pp. 2295-2298. doi: 10.5923/j.ajmms.20241409.36.
1. Introduction
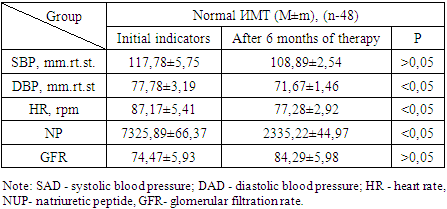
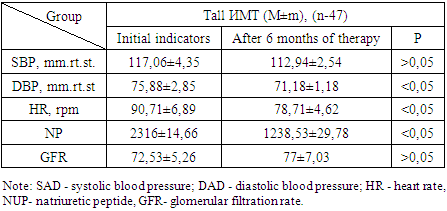
- A vulnerable phase of heart failure can occur with any BMI, but the risks and outcomes will vary. With obesity, patients often develop acute exacerbations of the disease, requiring hospitalization due to decompensation of cardiac function. At the same time, patients with a normal BMI may experience less acute deterioration, but are not immune from disease progression. To study the effect of empagliflozin on intracardiac and height-weight parameters and body composition before and after administration of the SGLT-2 inhibitor in patients in the vulnerable phase with heart failure with different body mass index. The initial characteristics of the patients included in the study are presented in Table 1. The data were collected upon admission to the hospital.
|

|
|
|
|
2. Materials and Methods
- Since ancient times, obesity has accompanied human life, and the attitude towards it is ambiguous. If Hippocrates wrote in his scientific works in 2400 BC that overweight people live a short life, and overweight women are infertile, In the XVIII–XIX centuries, the first scientific medical works devoted to this problem appeared. Since the beginning of the 20th century, with the rapid urbanization of the population, the popularization of high-calorie fast food in conditions of increasing physical inactivity, the proportion of the overweight population has also been growing. The study of the causes of obesity and its negative impact on human health begins. Major epidemiological studies of the last century have demonstrated that the consequences of obesity are such serious diseases as diabetes mellitus (DM), arterial hypertension (AH), coronary heart disease (CHD), chronic heart failure (CHF), impaired cerebral circulation [3,4,5]. In developed countries, cardiovascular diseases have become the leading cause of death. In the study Dudina A. and co-author. [6], completed and published in 2011, the SCORE scale (Systematic Coronary Risk Evaluation) was used to identify the correlation between body mass index (BMI) and traditional risk factors for cardiovascular diseases, such as age, smoking, total blood cholesterol, systolic blood pressure. The data included 12 cohort European studies, the analysis of which concluded that an increase in BMI for every five units correlated with an increase in cardiovascular mortality by 34% in men and 29% in women. Based on these data, the Specialized Center for Disease Control (Centers for Disease Control) in the United States predicted the development of an epidemic of overweight and the associated increase in cardiovascular diseases [1]. In 1982 Degoulet P. [7] for the first time publishes data that the presence of obesity does not worsen the prognosis of survival in patients undergoing hemodialysis.
3. Results and Discussions
- During 5 years of follow-up of 1,453 patients treated in 33 dialysis centers in France, there was no increase in mortality with a high BMI. 17 years later, the first prospective clinical trial appeared. In 1999, a nephrologist from the USA, Kalantar-Zadeh [8], observed 1,346 patients receiving hemodialysis for a year. For each unit of an increase in BMI of more than 27.5 kg/m2, the risk of mortality decreased by 6%, with a decrease in BMI of less than 20 kg/m2, the risk of mortality increased 1.6 times. The results remained significant after adjusting for blood albumin, transferrin and creatinine levels. In 2003, the same scientist proposed the term "reverse epidemiology", or "the obesity paradox". Over the past 5-6 years, there has been evidence that people with overweight (BMI 25-29.9 kg/m) and grade I obesity (BMI 30-34.9 kg/m2) have a longer life expectancy than people with normal weight. In Hassani et al. [9] publish the results of their observations: in overweight patients with coronary artery disease who underwent endovascular treatment of coronary arteries, the percentage of restenosis and mortality from cardiovascular causes is significantly lower than in patients with normal body weight. In, George D. Lundberg et al. [12] confirm that in patients with CHF, the presence of obesity does not worsen the cardiovascular prognosis: overweight correlates with a decrease in overall mortality by 25%, and with grade I obesity (these patients in the general population make up 80% of all obese people), the risk of death decreases by 12%. The phenomenon of the "obesity paradox" has strengthened its position. In our study, the 2nd group consists of patients with high BMI and low TMT. The reason for low lean body weight with a high body mass index in heart failure may be a metabolic disorder. Heart failure affects the functioning of the heart, which leads to insufficient supply of oxygen and nutrients to organs and tissues. This can cause decreased appetite, impaired digestion, and increased breakdown of proteins and muscles. Also, with heart failure, there may be fluid retention in the body, especially in the abdominal cavity and lower extremities. This can lead to an increase in body mass index due to water retention, but this liquid is not a lipid mass and does not provide normal nutrition to the body. In addition, with heart failure, muscle weakness and fatigue may occur, which can lead to a decrease in physical activity and, as a result, a decrease in muscle mass. All these factors together can lead to low lean body weight with a high body mass index in heart failure. A special group among patients with CHF mortality are those who have progressive weight loss. The estimated incidence of cachexia, defined as unintentional weight loss of more than 5% of total body weight in the previous 3-12 months, ranges from 13.3% to 16%. During 18 months of follow-up, mortality among such patients reaches 50%. Cachexia, as defined at the consensus conference on this condition in Washington in 2008, is characterized not only by weight loss, but also by concomitant symptoms such as fatigue, depression and anemia, which are associated with chronic diseases in the patient [1,10,11]. There are several theories about the mechanisms leading to the development of SC in patients with CHF, including malnutrition, activation of the immune system, imbalance between catabolic and anabolic processes, activation of the neurohumoral system and involvement in proinflammatory cytokines. In recent years, newly discovered hormones such as leptin, ghrelin and adiponectin, which regulate appetite and metabolism, have aroused interest. According to modern ideas about the pathogenesis of CHF, activation of neurohumoral systems plays a key role in the progression of CHF and SC, regardless of their causes. Some patients develop an inflammatory syndrome that activates the cytokine system, which, according to some studies, is associated with increased activity of the sympathoadrenal system [1]. The development of SC in patients with CHF occurs in the context of chronic inflammatory syndrome and has an unfavorable prognosis, regardless of the severity of the disease, the patient's age, his exercise tolerance and left ventricular myocardial contractility. Currently, the assessment of the degree of exhaustion is limited to the quantitative measurement of muscle mass using visualization and functional tests. However, these methods are expensive and available only in specialized medical institutions. Moreover, they make it possible to identify existing atrophy, but not the risk of its development. Therefore, one of the key areas of further research is to identify reliable biomarkers for early diagnosis and evaluation of the effectiveness of treatment, which at the same time will not be so costly. The main biomarkers with potential prognostic value and proposed for the assessment of SC are ethogrelin, adiponectin, the C-terminal fragment of agrin, growth and differentiation factor 15, atrial natriuretic peptide, N-terminal propeptide of collagen III, N-terminal globular domain of collagen epitope VI and myostatin [1,13,14].
4. Conclusions
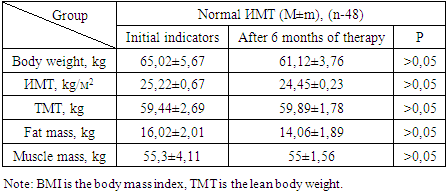
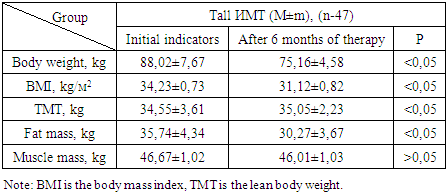
- In patients with CHF with increased BMI, the decrease in body weight was reflected by hyperhydration and an increase in lean body weight was noted. Thus, empagliflozin may have a positive effect on cardiac cachexia, improving metabolism, appetite and muscle mass in patients with heart failure. The effect of empagliflozin on lean body weight requires further research.