-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(8): 2042-2046
doi:10.5923/j.ajmms.20241408.21
Received: Jul. 22, 2024; Accepted: Aug. 16, 2024; Published: Aug. 22, 2024

Pathomorphological Changes in Blood Vessels of Pulmonary and Intestinal Mesenteric Arteries in COVID-19 Infection
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLHamza Nurmatovich Boboyev, Allaberganov Dilshod Shavkatovich, Amonov Shahrukh Rakhimovich
Department of Pathological Anatomy, Tashkent Medical Academy, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

In the period after the COVID-19 pandemic, the SARS-CoV-2 pathogen caused a nonspecific response of most organs and tissues. In particular, blockade of the APF-2 receptor in the arteries of the lung and mesentery was manifested by the development of acute dystrophic and necrotic changes, respiratory distress syndrome and acute intestinal failure, derailing the principle of blood vessel nutrition in the organs. Specific principles of morphological changes in the blood vessels of the lungs and mesentery were studied in the autopsies of those who died with the diagnosis of COVID-19. Changes in the endothelial area of the components of the blood vessel wall were studied. In the course of studies, it was found that thrombi develop as a result of severe swelling and desquamation of endotheliocytes.
Keywords: COVID-19, Pathomorphology, Pulmonary artery, Intestinal artery, Thrombosis, Endothelium
Cite this paper: Hamza Nurmatovich Boboyev, Allaberganov Dilshod Shavkatovich, Amonov Shahrukh Rakhimovich, Pathomorphological Changes in Blood Vessels of Pulmonary and Intestinal Mesenteric Arteries in COVID-19 Infection, American Journal of Medicine and Medical Sciences, Vol. 14 No. 8, 2024, pp. 2042-2046. doi: 10.5923/j.ajmms.20241408.21.
Article Outline
1. Introduction
- During the pandemic, death from thromboembolic complications after coronovirus infection is observed a lot (data from SSV RPAM 2021). Pulmonary edema develops as a result of interstitial edema in the alveolar wall of the lung tissue and the development of the thrombosis process in the capillaries. This, in turn, leads to many complications due to the increase of hydrostatic and oncotic, osmotic pressure in the blood vessels of the lung tissue. It is manifested in the lung tissue in the form of respiratory distress syndrome [1]. Clinical morphologically, it is manifested in the form of shortness of breath, wheezing, and continues for 6-8 hours with the formation of interstitial swellings in the alveolar walls and hyaline protein structures in the alveolar spaces. These same changes have also been found to develop in other organs [2]. However, lung tissue is one of the most dangerous organs among the vital organs, which manifests itself in the form of acute respiratory failure. Mortality in patients depends on age, gender and constitutional structure and develops differently [3]. It is precisely in the infection of COVID-19 that the blockade of the APF-2 receptor located in the vascular endothelium is manifested by dilatation of the vessel and the development of interstitial edema in the subendothelial layer and desquamation of endothelial cells.Purpose: to study the morphological changes in the pulmonary tissue and intestinal blood vessels and capillaries, alveolar walls and spaces, and to develop guidelines for clinical morphological diagnosis during coronavirus infection.
2. Materials and Methods
- Research materials were obtained from 32 autopsy results of patients who died of coronavirus infection at the Republican Pathological Anatomy Center of the Ministry of Health of the Republic of Uzbekistan in 2020-2021. Gross morphological examination by hematoxylin and eosin staining, the obtained materials are fixed in glutaraldehyde, contrasted with osmium 4 oxide, and frozen in epon blocks. Then, they are cut on an ultramicrotome and the obtained micropreparations are stained with methylene blue and picrofuscin. The obtained data are examined morphologically, and clinical anamnestic analysis is carried out from the history of the disease. Then the obtained data will be statistically analyzed.
3. Research Results and Their Discussion
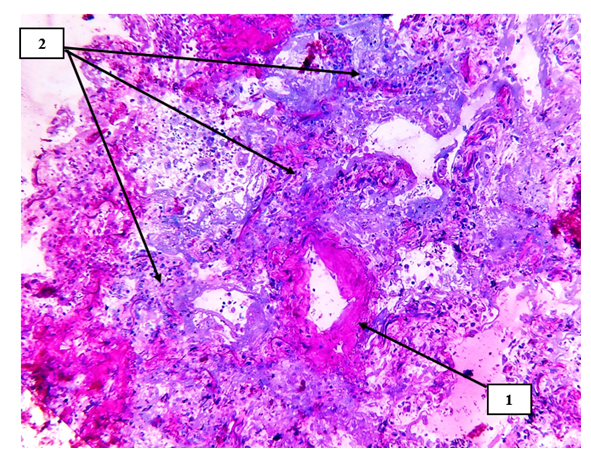
- In our study, lung tissue and intestinal mesentery are damaged to varying degrees in small-caliber blood vessels, directly related to hemodynamics and blood rheological indicators, and it is constitutionally that the sick contingents with high body weight with COVID-19 infection are clinically and morphologically small. In caliber blood vessels, blood circulation slows down and endothelial cells are damaged due to infection [4]. If the damage is observed in the arterial blood vessels entering the organs, it ends with the development of acute ischemia and necrosis of these organs. If the damage develops in the intima of the venous blood vessels, especially in the postcapillary venules, the occurrence of hydropic dystrophy and desquamation of endothelial cells leads to the development of primary thrombi in this area (see Fig. 1).
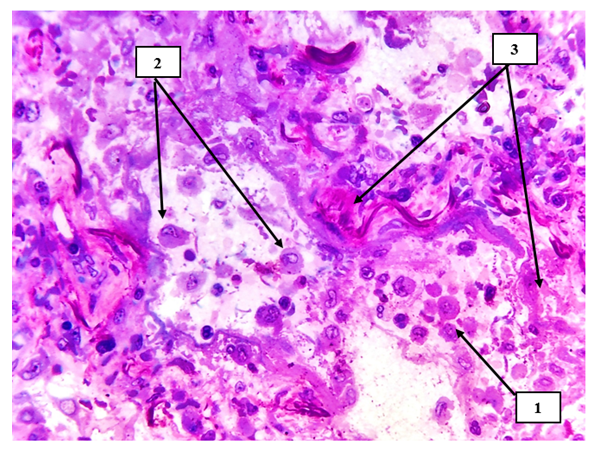 | Figure 1. Lung tissue. Macrophages with metaplastic giant cells are detected in the alveolar spaces (1), primary alveolar cells are also desquamated (2), sclerotic changes and coarse fibrous connective tissue structures are detected around small-caliber arteries (3). Semi-thin section. Stain methylene blue and picrofuscin. The size is 40x10 |
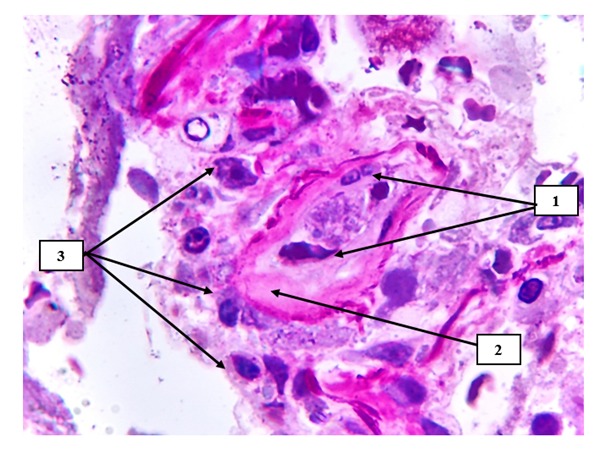 | Figure 2. Hyperchromic staining of endotheliocytes with a granular appearance on the surface of the pulmonary vascular endothelium (1), hyalinosis and pericytic area fibromatosis are detected in the vascular wall (2), chaotic arrangement of most macrophages (3). Semi-thin section. Stain methylene blue and picrofuscin. The size is 40x10 |
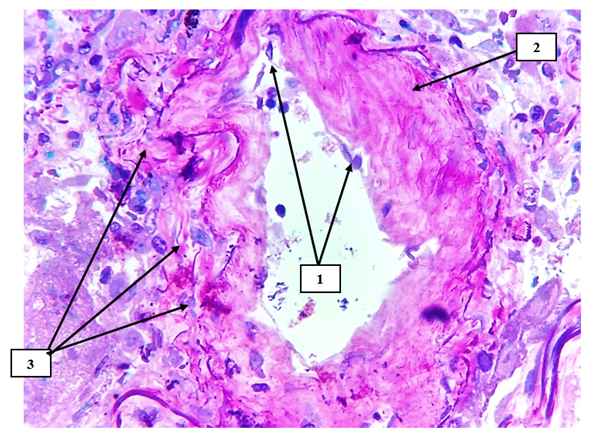 | Figure 3. Pulmonary tissue small-caliber artery. Desquamation of endotheliocytes on the surface of the arterial intima (1), hyaline uneven protein structures are detected on the vessel wall (2), irregularly migrated foci of lymphocytes and macrophages are detected on the sharply deformed surfaces of the perivascular relief (3). Semi-thin section. Stain methylene blue and picrofuscin. The size is 40x10 |
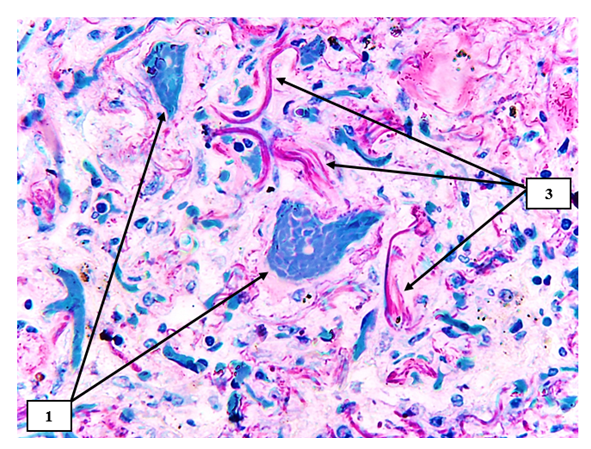 | Figure 4. Lung tissue. The histiotopography of the alveolar walls has changed, a small-caliber blood vessel with thrombosis consisting of erythrocytes is detected in the center and on the left (2). Various irregular fibrous structures with sparse fibers are identified (3). Semi-thin section. Stain methylene blue and picrofuscin |
 | Figure 5. Pulmonary tissue is a small-caliber blood vessel. The vascular wall is thickened, the vascular wall is sclerotized (1), the alveolar histiarchitectonics is changed, and foci of carnification after productive inflammation are identified (2). Semi-thin section. Stain methylene blue and picrofuscin |
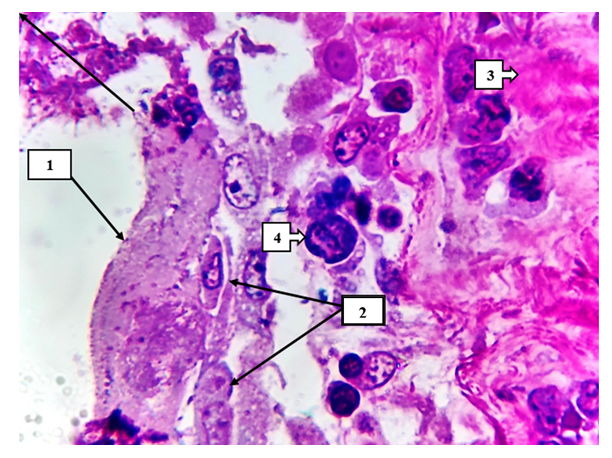 | Figure 6. On the inner surface of the alveolar wall, hyaline protein (1), dystrophic and necrobiotic changes of alveolocytes are detected (2). On the right are pink carnified foci (3). Macrophages with giant metaplasia are identified in the interval (4). Semi-thin section. Stain methylene blue and picrofuscin |
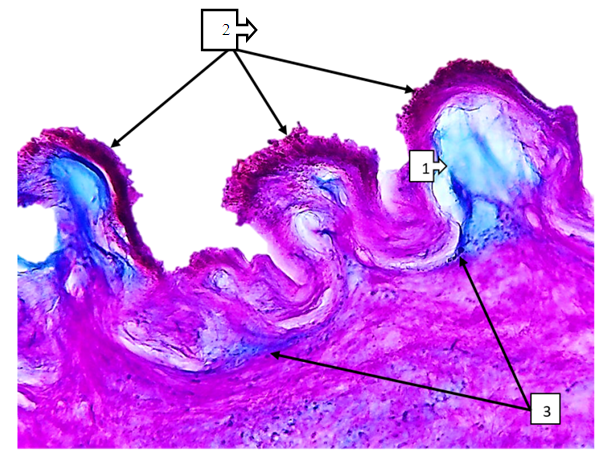 | Figure 7. Superior mesenteric artery in COVID-19. In the subendothelial space, there is a sharp accumulation of ShIFF-positive structures and mucoid discharge (1), and on the surface of the intima layer, thrombus aggregation is detected in a large and small granular form (2). The trajectory of the basal layer varies in thickness and appears thickened (3). Paint SHIFF paint. The size is 60x10 |
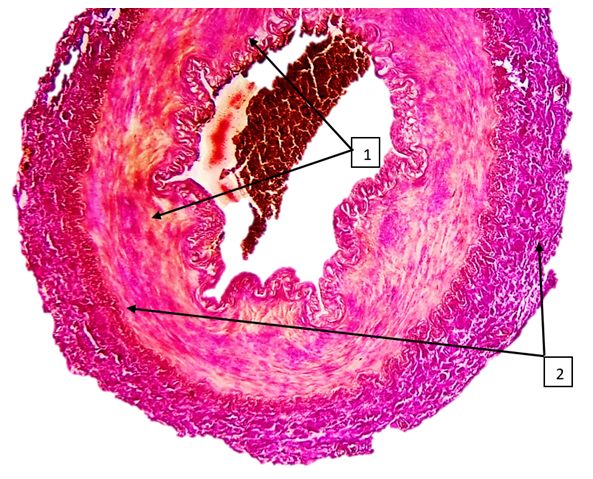 | Figure 8. Superior mesenteric artery in COVID-19. An uneven joule of fuchsinophilic fibers is found in the middle layer, and foci of irregularly located rough collagen fibers are identified in the muscle layer (2). The paint is Van Gison paint. The size is 10x10 |
4. Conclusions
- 1. Vacuolar dystrophy and desquamation of the endothelial cells of the vascular wall occur in COVID-19.2. It is determined that the migration of endothelial cells in the walls of blood vessels, which are rich in muscle fibers, is more frequent than in blood vessels of elastic type.3. It is characterized by the development of interstitial swelling in the subendothelial layer of blood vessels of the muscular type, and the sharp narrowing of the vascular space in the contracted state of the muscles and the occurrence of acute ischemic necrosis in the organs fed by this blood vessel.4. From a clinical morphological point of view, the deformation of small-caliber blood vessels, the surrounding of narrowed vascular spaces with tissue and cell components with thromboplastins is manifested in the transient ischemic or infarcted form as a result of acute vascular occlusion.5. Carnification of lung tissue and metaplasia of interstitial macrophages due to productive inflammation of lung tissue in interstitial pneumonia after COVID-19. These changes increase the likelihood of developing tumor diseases in the future.6. In COVID-19, the increase of Schiff-positive structures in the wall of the renal artery in various degrees leads to the development of interstitial edema and changes in the vascular relief. Changes in the vascular relief lead to changes in the folds of the endothelial surface, and mechanical damage of the endothelium under the influence of turbulent flow on the surfaces of large folds is an important factor for the formation of thrombus.