Аxmedov X. S.1, Ruzmetova I. Ya.2, Xalmetova F. I.1
1Tashkent Medical Academy, Tashkent, Uzbekistan
2Urgench Branch of Tashkent Medical Academy, Urgench, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Today, the role of vitamin D deficiency in rheumatic diseases has received much attention in recent years. It is known that the deterioration of the joint structure due to the disturbance of bone metabolism in rheumatic diseases significantly worsens the quality of life and prognosis of patients. In particular, a statistically significant superiority of patients with signs of osteopenia in rheumatoid arthritis, which is a representative of autoimmune diseases, was noted.
Keywords:
Rheumatoid arthritis, Vitamin D, Joints syndrome
Cite this paper: Аxmedov X. S., Ruzmetova I. Ya., Xalmetova F. I., Features of Articular Syndrome Against the Background of Vitamin D Deficiency in Rheumatoid Arthritis, American Journal of Medicine and Medical Sciences, Vol. 14 No. 8, 2024, pp. 2038-2041. doi: 10.5923/j.ajmms.20241408.20.
1. Introduction
Even in the second decade of the 21st century, rheumatic diseases continue to attract the attention of all aspects of medicine, and rheumatoid arthritis (RA) occupies one of the leading positions with its wide distribution [4]. According to information given in various sources, its share is 1-5%. This disease determines the social importance and urgency of the problem, as a specific joint syndrome differs from other joint diseases, causing structural disorders and functional disability in young and middle-aged patients. Today, the role of vitamin D deficiency in rheumatic diseases (RD) has received much attention in recent years [1,3]. It is known that the deterioration of the joint structure due to the disturbance of bone metabolism in RD significantly worsens the quality of life and prognosis of patients. In particular, a statistically significant superiority of patients with signs of osteopenia in RA, which is a representative of autoimmune diseases, was noted [2,9].Purpose: To assess the value of a method for detecting early remodeling of the joint structure due to vitamin D deficiency in patients with rheumatoid arthritis.
2. Research Material and Methods
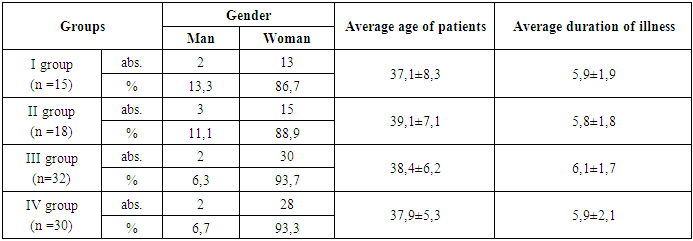
95 randomly selected patients with RA, aged 18-49 (38.1±13.3), with an average duration of 6.1±1.9 years, were involved in the research. Among them, the main share - 76 (80%) was accounted for by women. To carry out the study, patients with RA were divided into four groups, group I - in the range of "70-100 ng/ml" without vitamin D deficiency (n=15) [8]; Group II - vitamin D deficiency was not observed in the range "30-70 ng/ml" (n=18); Patients with group III - vitamin D "suboptimal status - 10-29 ng/ml" (n=32) and group IV - vitamin D "deficiency status -10 ng/ml" were included (n=30). For the control group, 20 healthy individuals (mean age 37.2±7.1 years) were selected, and they were roughly matched with the groups of RA patients by age and gender (Table 1).Table 1. Clinical characteristics of RA patients (n=86)
 |
| |
|
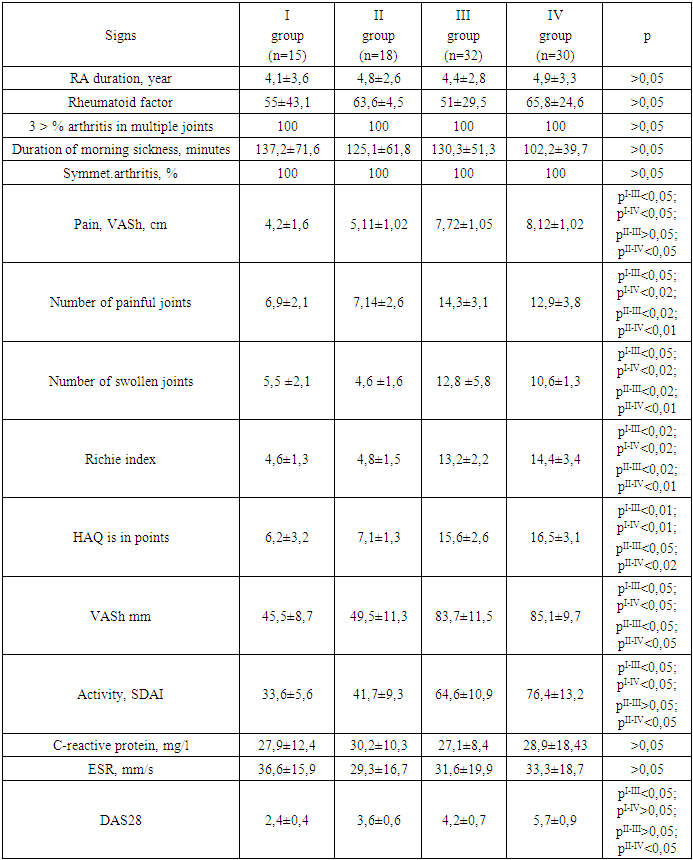
Determination of the clinical course and activity of RA was performed by evaluating the visual analog scale (VASh), DAS28 and acute phase indicators of inflammation [9]. Functional classes (FS) and the Stanford Health Assessment Questionnaire (HAQ) were used to evaluate the functional capabilities of patients [6]. Laboratory examination included general clinical and biochemical blood tests. X-ray, UTT and MRI examination of joints was performed in all patients. Bone metabolism was studied using pyridinoline and bone isozyme of alkaline phosphatase using enzyme immunoassay method [13].The obtained results and their discussion. 66.9% of the patients involved in the study were 30-45 years old, and 80% were women. Based on the analysis of the data in the anamnesis of the disease, the average age of the patients at the time of the first symptoms of RA was 29.9±4.9. The average period between the appearance of the first symptoms and the diagnosis was 9.5 ± 3.6 months.According to the obtained results, the clinical appearance of RA was different from each other in four groups. Patients with RA of groups III and IV differed from patients of groups I and II with a clear clinical picture of joint syndrome. As can be seen from Table 2, the average number of swollen and painful joints in them was significantly higher than that of patients in groups I and II (p<0.05), i.e. 2 times more. In turn, the duration of morning sickness did not differ statistically significantly (r>0.05) between groups. Inflammatory markers - C-reactive protein and erythrocyte sedimentation rate (ESR) were high in all groups and were not statistically significantly different, but activity indices SDAI and DAS28 had higher values based on vitamin D deficiency.Table 2. Clinical presentation of patients with RA
 |
| |
|
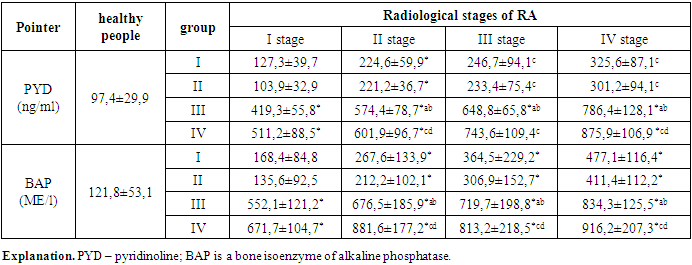
At this point, it should be said that group I of patients with RA, i.e., vitamin D in their blood serum in an intermediate situation of "70-100 ng/ml", differed from other groups of patients according to the DAS28 index. In addition, a significant and obvious difference was found according to the HAQ and Rich index (p<0.05), which means that the functional ability of the joints was limited due to vitamin D deficiency (groups III and IV).Assessment of the development of the joint syndrome showed early damage of the proximal interphalangeal and metatarsophalangeal joints of the hands in the early stages of the disease in all groups. However, over time, other joint damage was distinguished by serum vitamin D levels in patients.It is known that vitamin D deficiency has a direct effect on bone metabolism. For example, since calcium and phosphorus penetration into bone depends on vitamin D, it is of practical importance to assess the balance of resorptive and osteogenesis processes in bone [5,7]. In the RA patients included in the study, these parameters indicated that there were specific differences between the groups.Signs of reliability between groups (r<0.05): "*" - when compared with the indicator of healthy people; "a" - between groups I and III; "b" - between II and III groups; "c" - between groups I and IV; "d" is a symbol between groups II and IV.Table 3. The bone metabolism indicators in patients with RA
 |
| |
|
As can be seen from Table 3, the bone metabolism indicators changed with the progression of the radiological (R°) picture of the disease in patients with RA. In particular, there were no statistically significant differences (r>0.05) in patients without pyridinoline (PYD) vitamin deficiency [11,12], that is, in the R°-I stage of RA in groups I and II. However, it was found that PYD in these groups increases reliably (r<0.05) starting from stage II of RA. On the other hand, in patients with vitamin D deficiency (groups III and IV), PYD clearly increased from the early stages of the disease [10,15], that is, in the R°-I stage, and it differed by almost 4-5 times compared to healthy people. Moreover, PYD increased as the disease R° progressed, and the rate was significantly higher in this group than in groups I and II [14].
3. Conclusions
Thus, in patients with RA, there is an increase in the amounts of pyridinoline and alkaline phosphatase bone isoenzymes in joint tissue formed on the basis of vitamin D deficiency from the early stages of remodeling.
References
| [1] | Aslam M. M. et al. Vitamin D as a principal factor in mediating rheumatoid arthritis-derived immune response // BioMed Research International. – 2019. – Т. 2019. |
| [2] | Cutolo M. et al. Vitamin D in rheumatoid arthritis // Autoimmunity reviews. – 2007. – Т. 7. – №. 1. – С. 59-64. |
| [3] | Hajjaj-Hassouni N. et al. Evaluation of vitamin D status in rheumatoid arthritis and its association with disease activity across 15 countries: “The COMORA Study” // International journal of rheumatology. – 2017. – Т. 2017. |
| [4] | Harrison S. R. et al. Vitamin D and early rheumatoid arthritis // BMC rheumatology. – 2020. – Т. 4. – С. 1-7. |
| [5] | Heidari B., Hajian-Tilaki K., Babaei M. Vitamin D deficiency and rheumatoid arthritis: epidemiological, immunological, clinical and therapeutic aspects // Mediterranean journal of rheumatology. – 2019. – Т. 30. – №. 2. – С. 94-102. |
| [6] | Higgins M. J. et al. The effect of vitamin D levels on the assessment of disease activity in rheumatoid arthritis // Clinical rheumatology. – 2013. – Т. 32. – С. 863-867. |
| [7] | Ishikawa L. L. W. et al. Vitamin D deficiency and rheumatoid arthritis // Clinical reviews in allergy & immunology. – 2017. – Т. 52. – С. 373-388. |
| [8] | Leventis P., Patel S. Clinical aspects of vitamin D in the management of rheumatoid arthritis //Rheumatology. – 2008. – Т. 47. – №. 11. – С. 1617-1621. |
| [9] | Lin J. et al. Serum vitamin D level and rheumatoid arthritis disease activity: review and meta-analysis //PloS one. – 2016. – Т. 11. – №. 1. – С. e0146351. |
| [10] | Meena N. et al. Assessment of vitamin D in rheumatoid arthritis and its correlation with disease activity // Journal of natural science, biology, and medicine. – 2018. – Т. 9. – №. 1. – С. 54. |
| [11] | Song G. G., Bae S. C., Lee Y. H. Association between vitamin D intake and the risk of rheumatoid arthritis: a meta-analysis // Clinical rheumatology. – 2012. – Т. 31. – С. 1733-1739. |
| [12] | Sukharani N. et al. Association between rheumatoid arthritis and serum vitamin D levels // Cureus. – 2021. – Т. 13. – №. 9. |
| [13] | Yang J. et al. Effect of vitamin D on the recurrence rate of rheumatoid arthritis // Experimental and therapeutic medicine. – 2015. – Т. 10. – №. 5. – С. 1812-1816. |
| [14] | Akhverdyan Yu. R. et al. Relationship between bone remodeling markers and bone fracture risk in patients with rheumatoid arthritis // Yakut medical journal. - 2021. - No. 2. - P. 120-122. |
| [15] | Dedov D. V. Secondary osteoporosis in patients with rheumatoid arthritis, prevention of complications with the help of Osteomed, Osteomed Forte, Osteo-Vit D3 // Pharmacy. - 2022. - V. 71. - No. 3. - P. 5-9. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML