-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(8): 2000-2003
doi:10.5923/j.ajmms.20241408.12
Received: Jul. 17, 2024; Accepted: Aug. 3, 2024; Published: Aug. 10, 2024

Clinical Features of Intracted Ventral Hernias Complicated by Intestinal Obstruction
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLUtaev Latif Kholmamatovich1, Dusiyarov Muhammad Mukumbayevich2, Askarov Pulat Azadovich2, Khujabaev Safarboy Tukhtabayevich2
1Navoiy Branch of the Republican Emergency Medical Care, Uzbekistan
2Samarkand State Medical University, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The study used retrospective and prospective data of 242 patients who had surgeries for incarcerated hernias of the anterior abdominal wall complicated by intestinal obstruction. Regardless of the type and size of incarcerated ventral hernias, high intra-abdominal pressure (IAP) with the risk of enteral and multiple organ failure is an indication for the use of tension-free methods of plastic surgery. SPK can be prevented by enteral intubation. In the main study group, a significant (p<0.05) tendency to decrease IAP as a result of tension-free plastic surgery and enteral intubation was found. In the comparison group, the initial value of 19.3±1.6 decreased to 17.1±1.3 after surgery, and in the main group, the initial value of 18.8±1.8 decreased to 14.5±1.3 mm Hg. Resolution of intestinal paresis and obstruction can be effectively monitored using abdominal ultrasound.
Keywords: Strangulated ventral hernias, Intestinal obstruction
Cite this paper: Utaev Latif Kholmamatovich, Dusiyarov Muhammad Mukumbayevich, Askarov Pulat Azadovich, Khujabaev Safarboy Tukhtabayevich, Clinical Features of Intracted Ventral Hernias Complicated by Intestinal Obstruction, American Journal of Medicine and Medical Sciences, Vol. 14 No. 8, 2024, pp. 2000-2003. doi: 10.5923/j.ajmms.20241408.12.
1. Introduction
- Treatment of strangulated hernias of the anterior abdominal wall is one of the important areas of emergency surgery, which receives much attention in research and publications. These hernias complicate the course of the disease in 10-17% of patients with hernias and rank second among acute surgical diseases of the abdominal organs after acute appendicitis. However, mortality from strangulated hernias is 15-16 times higher than from acute appendicitis. Statistics from leading research and medical institutions show that, despite achievements, surgical treatment of patients with strangulated abdominal wall hernias gives unsatisfactory results. Postoperative complications reach 50%, and mortality ranges from 2 to 4 percent. This is due to the high frequency of strangulation of intestinal loops, leading to strangulation intestinal obstruction (more than 70%), as well as a large number of elderly patients (about 40%).
2. Materials and Methods
- Incorrect choice of the method of plastic surgery, significant tension of the abdominal wall tissues, decrease in the volume of the abdominal cavity and development of abdominal compartment syndrome in 0.8-12% of operated patients are the main reasons for unsatisfactory results of the operation. Purpose of the study. Development of a strategy for diagnosis and operations for strangulated ventral hernias complicated by intestinal obstruction, including the choice of the method of hernioalloplasty. Materials and methods. The work is based on the results of a retrospective and prospective study of 242 patients operated on for strangulated hernias of the anterior abdominal wall of various localizations complicated by the development of intestinal obstruction, who were in patients at the Navoi branch of the RNCEM in 2018- 2023. Patients were subjected to clinical observation, who were divided into two groups depending on the nature and scope of the surgical intervention. The main group consisted of 136 patients with strangulated hernias of the anterior abdominal wall complicated by intestinal obstruction, who underwent surgery using synthetic implants (the method of "tension-free" hernioplasty). This group included patients with different localizations of hernias: 46 (33.8%) with strangulated inguinal hernias, 38 (27.9%) with strangulated umbilical hernias and 52 (38.2%) with strangulated postoperative ventral hernias.The control group included 106 patients with strangulated hernias of the anterior abdominal wall complicated by intestinal obstruction, who underwent traditional autoplasty operations ("tension" hernioplasty). This group also consisted of patients with different localizations of hernias: 30 (28.3%) with strangulated inguinal hernias, 34 (32.1%) with strangulated umbilical hernias and 42 (39.6%) with strangulated postoperative ventral hernias. In the main group, the average age of patients was 56.4 years (plus or minus four years), with an age range from 28 to 81 years. Among them, there were 74 women (54.4%) and 62 men (45.6%). In the control group, the average age of patients was 57.6 (plus or minus 3.1) years, and the age range was from 27 to 78 years. There were 50 men (47.2%) and 56 women (52.8%).
3. Result Discussion
- Most of the surgical patients in the older age group had serious comorbidities that affected the course and outcome of the disease. 82% of people in this age group had 2-3 comorbidities. According to the anamnesis, the duration of wearing a hernia before admission to the hospital varied from 1 to 20 years, with a total duration of 9.5 + 1.7 years.From the onset of strangulation, patients admitted to the emergency department of the Samarkand branch of the RRCEM had different periods. The hospitalization time in the main group ranged from 4 to 144 hours, with a total duration of 27.1 plus or minus 8.4 hours. Six patients (8.8%) were admitted within the first six hours; 46 (33.8%) were admitted between six and twelve hours; 38 (27.9%) were admitted between twelve and twenty-four hours; and 20 (29.4%) patients were admitted after strangulation after 24 hours.The hospitalization time in the control group ranged from 3 to 144 hours, with a mean stay of 22.6 plus or minus 6.8 hours. Six patients (11.3%) were admitted within the first six hours; 42 (39.6%) were admitted between six and twenty-two hours; 30 (28.3%) were admitted between twenty-two and twenty-four hours; and 22 (20.8%) were admitted after 24 hours from strangulation.238 (98.3%) patients reported that their previously freely reducible hernia could not be treated. They also reported that the hernia was becoming more painful and increasing in size. In 230 patients (95.1%), no "cough impulse" was observed during palpation. Nausea was observed in 136 (55%) patients, vomiting, which recurred at the prehospital stage and periodically recurred in 92 (37%) patients, delayed passage of stool and flatus in 64 (26%) patients, and increased peristalsis in 34 (14%) patients. 28 (11%) patients showed peritoneal symptoms, and 10 (4%) patients noted a change in skin color over the hernial protrusion.Radiographic examination was performed in 188 (75%) patients admitted to the hospital who had an incarcerated hernia of the anterior abdominal wall, which was complicated by intestinal obstruction. Abdominal radiographs showed that 53.1% of patients had evidence of low small bowel obstruction with multiple horizontal fluid levels in dilated small bowel loops. 26.6% of patients had evidence of high small bowel obstruction on radiographs.
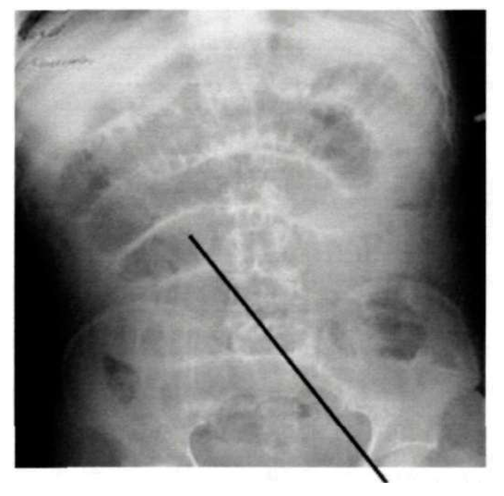 | Picture 1. Patient D., 51 years old. X-ray image of strangulated inguinal hernia with signs of small bowel obstruction (direct projection) |
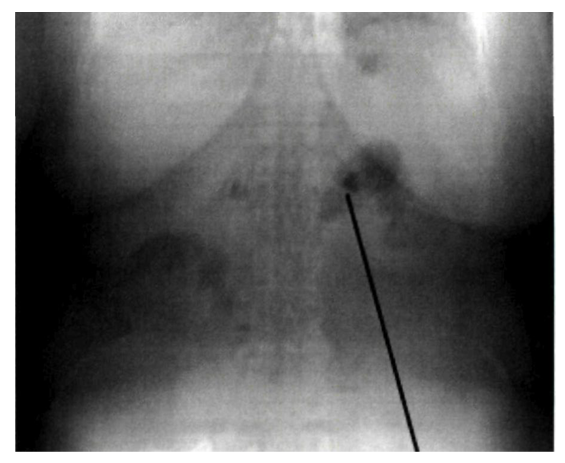 | Picture 2. Patient A., 63 years old. Postoperative ventral hernia with radiographic signs of intestinal obstruction (direct projection) |
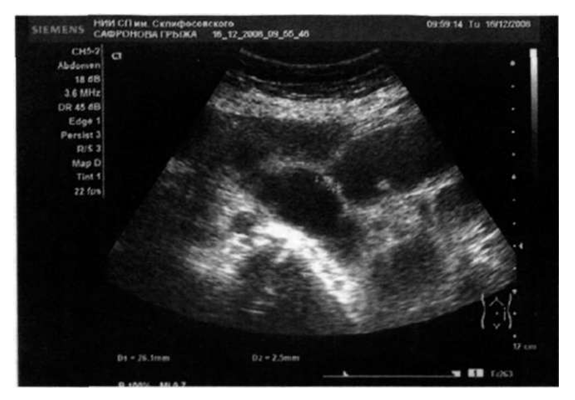 | Picture 3. Patient R., 52 years old. Ultrasound: strangulated ventral hernia: the hernial orifice is located, through which a fragment of the small intestine with liquid contents comes out, without peristalsis. Blood flow in the wall is not registered. Fluid in the hernial sac is located |
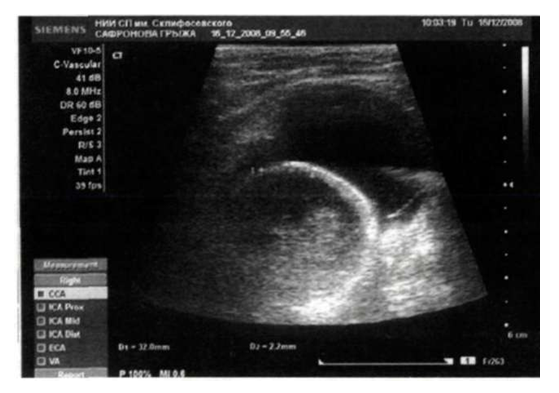 | Picture 4. Patient J., 71 years old. Ultrasound: Strangulated right-sided inguinal hernia: In the right inguinal region, a hernial orifice up to 1.5 cm is located, into which a fragment of the small intestine with a diameter of 3.2 cm emerges, the wall is 0.3-0.4 cm, blood flow in the wall and peristalsis are not recorded, the contents are liquid in nature. Heterogeneous hernial fluid is located |
4. Conclusions
- 1. In strangulated ventral hernias of any type and size, the use of tension-free methods of plastic surgery is indicated due to increased intra-abdominal pressure, which can lead to enteral and multiple organ failure. Intestinal failure syndrome can be prevented with endotracheal intubation.2. In the main study group, there was a significant tendency to decrease IAP (p<0.05) when using NEI and tension-free plastic surgery. In the comparison group, IAP dropped from the initial value of 19.3 ± 1.6 to 17.1 ± 1.3 mm Hg after surgery, while in the main group it dropped from 18.8 ± 1.8 to 14.5 ± 1.3 mm Hg with a similar trend over the next three days. Ultrasound examination of the abdominal cavity can effectively monitor the resolution of paresis and intestinal obstruction. 3. An algorithm for treating patients with strangulated hernias complicated by intestinal obstruction, taking into account the degree of enteral insufficiency, the level of IAP, the type and size of hernias, can reduce the incidence of abdominal complications from 20.7% to 4.4%, general postoperative complications from 28.3% to 11.3%, mortality from 5.2% to 1.5% and the incidence of wound complications from 28.3% to 8.8%.