Matrizaeva Kurbonbika Madrimovna, Yusupova Mekhribon Atakhanovna
Urgench Branch of the Tashkent Medical Academy, Urgench, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
In the structure of extragenital pathology during pregnancy, urinary tract infections are represented in second place after diseases of the cardiovascular system. Infectious and inflammatory urological complications and diseases pose a difficult problem for diagnosis and treatment. At present, there are no unified approaches to the problem of the BBU itself. Information about tactical measures is limited, unified algorithms for the management of pregnant women, including timely microbiological diagnosis and treatment of this condition, has not been worked out. This article provides a comprehensive overview of measures to reduce the complications that may result from asymptomatic bacteriuria.
Keywords:
Pregnancy, Asymptomatic bacteriuria, Bacteriospermia
Cite this paper: Matrizaeva Kurbonbika Madrimovna, Yusupova Mekhribon Atakhanovna, Prevention of Obstetric and Perinatal Complications in Pregnant Women with Asymptomic Bacteriuria, American Journal of Medicine and Medical Sciences, Vol. 14 No. 7, 2024, pp. 1897-1901. doi: 10.5923/j.ajmms.20241407.36.
1. Introduction
Asymptomatic bacteriuria in pregnant women is a microbiological diagnosis that is based on the examination of urine collected with maximum sterility. A feature of BBU is the complete absence of clinical signs of urinary system disease (dysuria, intoxication, etc.). Asymptomatic bacteriuria is observed 10 times more often in women than in men, and is detected in 2-10% of pregnant women. In most women, bacteriuria occurs before pregnancy. 20-40% of women develop acute pyelonephritis during pregnancy.A prerequisite for the upward spread of microorganisms is sexual activity [1-2]. In a woman's urinary tract infection, the husband's asymptomatic bacteriospermia is of great importance. In sexual partners suffering from a genitourinary tract infection, many bacteria are cultured from the semen. This explains Saturday or Sunday morning cystitis, which occurs in women a week after sexual intercourse with a partner suffering from asymptomatic bacteriospermia. Treatment of the sexual partner and the use of a condom reduces the number of recurrences of genitourinary tract infections in women [3-7].
2. Materials and Methods
The source of infection of the urinary tract is also inflammatory processes in the female genital organs and surrounding pelvic tissue, where bacteria can remain in a “dormant” state for a long time. With vulvitis and bacterial vaginitis, the ascending spread of microorganisms during pregnancy occurs especially often [8-9].During pregnancy, the anatomical and functional state of the urinary tract changes, manifested by expansion of the renal collecting system and insufficiency of the sphincter mechanism of the bladder. The development of bacteriuria is facilitated by factors arising from the effect of progesterone on the muscle tone of the ureters and their mechanical obstruction by the growing uterus. These include: a slowdown in the rate of urine passage due to a decrease in the tone and peristalsis of the ureters, expansion of the renal pelvis and upper parts of the ureters with the formation of physiological hydronephrosis of pregnant women, a decrease in urinary tone 15 bladder, an increase in the amount of residual urine, contributing to vesicoureteral reflux and upward migration of bacteria to the upper urinary tract. Existing hypotension and enlargement of the kidneys are detected by ultrasound and excretory urography [10-14].Hormonal changes during pregnancy contribute to physiological relaxation of the uterus and pathological relaxation of all parts of the urinary system [15-17]. Estrogens cause a hypertonic or hyperkinetic state of the urinary tract, progesterone leads to hypotension and hypokinesia. The excess of hormones in the blood serum in pregnant women coincides in time with the occurrence of disturbances in the urodynamics of the upper urinary tract and the development of pyelonephritis. Dilatation of the upper urinary tract in healthy women during pregnancy before 20 weeks is rare. A decrease in IgG in the blood serum at 21-22 weeks of pregnancy, in combination with hormonal incoordination and impaired urodynamics, contributes to a more frequent occurrence of ABU and pyelonephritis in pregnant women during these periods [1,4,18,19]. In the third trimester of pregnancy, the placenta begins to secrete large quantities of estrogens, progesterone and glucocorticoids. Estrogens promote the growth of bacteria pathogenic to the urinary organs, which is due in particular to a decrease in lymphocyte function [20].In 70-95% of cases, the main pathogen in UTI is E. Coli; other representatives of Enterobacteriaceae, such as Proteus spp, Klebsiella spp, are less often identified. etc. In nosocomial infections, the spectrum of isolated microorganisms is wider and, along with the above-mentioned enterobacteria, there is a decrease in the frequency of detection of E. Coli with an increase in the frequency of detection of Serratia spp., Morganella spp., Citrobacter spp., Pseudomonas aeruginosa, Staphyloccoccus aureus, enterococci [12,21-23]. According to the degree of uropathogenicity, microorganisms are divided into the following groups: - primary pathogenic - species that cause UTI in individuals without pathology. This group also includes rarely detected species of bacteria (Salmonella);- secondary pathogenic – species that rarely cause primary 17 infection in individuals without UTI pathology, but are associated with nosocomial UTI: Klebsiella spp., Enterobacter spp., Proteus vulgaris, Morganella, S. Aureus, Enterococcus spp., Candida albicans.The causative agents of UTIs also include anaerobic bacteria, fungi, myco- and ureaplasmas, viruses, trichomonas, L-form bacteria, when, with a temporary subsidence of the inflammatory process, urine cultures do not yield results [4].Thus, the main methods for diagnosing BBU are currently bacteriological, microscopic, chemical (test strips) and instrumental (ultrasound, MRI) methods. At the same time, the above emphasizes the need to find a new algorithm for diagnosing BBU in pregnant women.
3. The Purpose of the Study
To reduce obstetric and perinatal complications by optimizing the management of pregnant women with asymptomatic bacteriuria.
4. Research Result
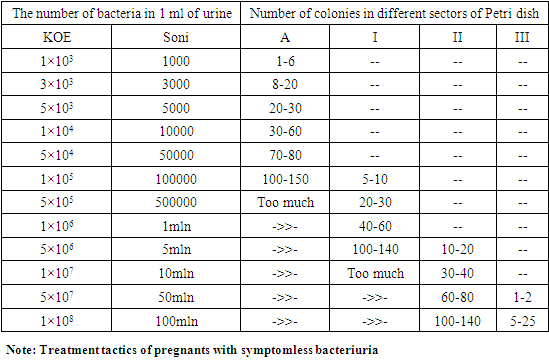
Scientific work was carried out in 2020-2022 at the Department of Obstetrics and Gynecology, Urganch branch of the Tashkent Medical Academy. The collection of clinical materials was carried out in the family polyclinic No. 1 and in the Perinatal Center of the Khorezm region, which is the clinical base of the department.84 women who applied to the center in order to achieve the goal of scientific work were observed. Depending on the type of treatment, women were divided into 3 groups.Main group 1 - (n-30) pregnant women and women who gave birth, whose husbands were diagnosed with asymptomatic bacteriuria during pregnancy and treated after bacteriological examination of urine.Comparison group 2 - (n-30) women whose asymptomatic bacteriuria was detected and treated according to anamnestic data, but pregnant women whose husbands were not examined.Control group 3 - (n-24) practically healthy pregnant women with normal urine bacterial analysis. Women not included in the study: women with chronic kidney disease, women with severe extragenital pathologies, women with coagulopathy.Clinical examination included obstetric and gynecological anamnesis, studies of diseases before pregnancy and during pregnancy. Obstetric examination was performed according to the generally accepted method (Leopold-Levitsky technique, listening to the heartbeat of the fetus, examination of the cervix and vagina using mirrors, bimanual examination). The cleanliness of the vagina was checked, bacteriological studies of the cervical canal were conducted to identify pathogenic flora and take preventive measures. During observation and treatment, all pregnant women underwent blood and urine tests. Total protein, blood bilirubin, sugar, urea and blood creatinine were studied. Analysis of urogenital infections. Ultrasound examination of the fetus and Doppler examination of the fetoplacental complex.To determine the nature of the microflora and their sensitivity, a bacteriological culture was planted and sensitivity to antibiotics was determined. Anatomical changes in the kidneys were determined using ultrasound. At the same time, expansion and hypotonic dyskinesia of the urinary tract and ureteral system were determined, the size of the kidneys, the thickness of the cortical layer, the size of the ureteral complex, and anatomical and functional disorders of urodynamics were determined. The upper urinary tract (hydronephrosis, developmental anomalies, stones, etc.) was examined. All pregnant women consulted a general practitioner, urologist, cardiologist and other specialists.Morphological, microscopic and biochemical properties were studied after 37 hours in a thermostat at 24 degrees Celsius. Biochemical properties of isolated microorganisms were evaluated in liquid medium: glucose-lactose-malinite-sucrose.In determining the sensitivity of microbes to antibiotics, the width of the bacterial growth zone became important (discs soaked in antibiotic solution were placed on the meat-peptone agar surface in a Petri dish).The effect of the antibiotic was evaluated by the duration of growth around the disc after incubation at 24 C in a thermostat for 37-18 hours.Depending on the diameter of the growth zone of the microflora, the level of sensitivity of the test strain to the antibacterial drug was distinguished. A growth zone diameter of more than 10 mm corresponded to hypersensitivity, less than 10 mm to sensitivity, and complete absence was considered resistant to this drug. The degree of contamination with pathogens in SB was determined by the number of colony-forming elements in 1.0 ml of urine.Table 1. Number of bacteria and colony-forming units in 1 ml of urine
 |
| |
|
Screening for asymptomatic bacteriuria in pregnant women in the first trimester is recommended: pregnant women with a concentration of 105 KOE/ml of the same pathogen in 2 consecutive urine samples collected during spontaneous urination (24 hours apart) in the urine bacteriological analysis was involved. The husbands of 30 women also agreed to submit the bacterial analysis of urine and sperm, and they were included in the first group. Husbands of pregnant women in group 2 did not submit urinalysis.Pregnant women in the 1st group were injected with fosfomycin trometamol 3 g once and phytopreparations containing cranberry fruit were prescribed 3 times for 1 month. Fosfomycin trometamol 3g was administered to their husbands 1 time. After treatment, no repeat urinalysis was obtained according to the national standard. Urinalysis for bacteriuria was performed in women only when symptoms of urinary tract pathologies were observed.Women in group 2 received fosfomycin trometamol 3 g only once. Husbands were not involved in the investigation and were not treated.No bacteriuria was observed in the urine of group 3 women and no treatment measures were taken.Women in all groups regularly took iodine preparations and polyvitamins that should be taken during pregnancy.The following types of statistical analysis were used for mathematical processing of the obtained data. Samples (p) According to the Student's test, the trend of statistically significant differences was obtained at the value of p≤0.05. Arithmetic mean value and its error (M±m) are shown.Research results: The age of the women in the study groups ranged from 18 to 35 years, with an average of 27 years. The examinees of group 1 were mainly women aged 18-24, in this group there were 4 women over 31 years old (13.4%), and in group 2 women were aged 18-30, and 4 women (13.4%) 16 (66.7%) women aged 18-24 and 8 (33.3%) aged 25-30 were women of the 3rd group. There were no women older than 31 years in this group. Women of all groups are mostly of reproductive age. Among the women older than 31 years, all of the 4 (13.4%) women in groups 1 and 2 were women who were trying to have children and were reproducing.Among the observed women, the incidence of acute respiratory diseases and influenza was high, and among the groups, 18 (60%), 20 (66.7%), 15 (62.5%) women were observed, respectively. Children's infections, chronic tonsillitis were more common in the first and second groups compared to the control group. The incidence rate of appendicitis did not differ much between the groups, it was 3(10%), 3(10%), 2(8.3%) people, respectively. The gastrointestinal tract did not differ much between the first and second groups. 2(6.7%) in the first group, 3(10%) in the second group, and 1(4.2%) in the control group. Varicose veins and hypothyroidism were equally observed in 2 (6.7%) and 1 (3.3%) women of the 1st and 2nd groups. Hepatitis B, C and AIDS were 3.3% among women of group 1, and among other observed women this pathology was not detected. Depending on the level of obesity, 2(6.7%), 4(13.3%), 1(4.2%), 2nd grade 2(6.7%), 4(13.3%), 3rd grade 1-2 groups respectively observed in 3.3% of cases.One of the indicators that attracted special attention was iron deficiency anemia, which occurred equally in all groups, 10 (33.3%), 5(16.7%), 1(4.2%), moderate in the mild groups, respectively. ir degree was found in 16 (53.3%), 13 (43.3%), 5 (20.8%) and 1 (3.3%) women in groups 1-2.During this pregnancy, three groups of women underwent blood analysis to detect TORCH infection, the reason for this was to clarify the idea that in most cases, infection in pregnancy pathologies leads to miscarriages, fetal growth failure, and perinatal losses. indicators were similar in the group, and it was found that the pregnancy pathologies that occur do not depend only on TORCH infection.Our observations showed that Toxoplasma Gondii-IgG and Chlamydia trachomatis-IgG were not detected in any of the three groups.Cytomegalovirus-IgG was 17(56.7%), 16(53.3%), 14(58.3%) of the groups. Rubella-IgG was detected in 14 (46.7%) women in the 1st group, 17 (56.7%) in the second group, 15 (62.5%) in the control group. Herpes Simpex-IgG was found to be the most common infection and was found in 20 (66.7%) patients in group 1, 18 (60%) in group 2, and 18 (75%) in group 3. Ureaplasma urealyticum-IgG appeared in the blood of 1 (3.3%) women in group 1, 3 (10%) in group 2, and 2 (8.3%) women in group 3.When the biocenosis of women's vagina was observed, the first degree purity of the vagina was not observed in women of the 1st and 2nd groups, and in the 3rd group only 2 (8.3%) pregnant women were found to have the first degree purity. Grade 2 purity was found in 20(66.7%), 18(60%) and 14(58.3%) individuals, respectively. Level 3 cleanliness was observed in 9(30%) of group 1, 12(40%) of group 2 and 7(33.3%) of group 3 (coccal bacteria). Grade 4 purity was observed only in 1 (3.3%) woman in group 1, and a large number of E.coli bacteria and mycelia were detected.In order to determine the causes of asymptomatic bacteriuria in pregnant women, in cooperation with the Department of Regional Sanitary Epidemiology and Public Health Service, we conducted tests such as bacteriuria in the urine of pregnant women and their husbands, determining the causative agent of bacteriuria and antibiotic sensitivity.According to the information we received from the Department of Regional Sanitary Epidemiology and Public Health Service, in 2020, 415 pregnant women submitted urine for bacteriuria, of which 82 (19.8%) women had a positive bacteriuria result, and in 2021, this the indicator was observed in 142 (26.2%) women out of 542.When comparing the type of bacteria in the urine of the examined women, E.coli was detected in many women in both groups, the number corresponding to the groups was 15 (50%), 16 (53.3%). The next most common bacterium is St. epidermidis, observed in 6 (20%), 5 (16.7%) people, respectively. It was determined that the risk of this bacterium is low due to the fact that it can form colonies and cause complications in pregnancy, even if it occurs in many women. Klebsiella pneumonia was detected equally in both groups of women, making up 6.7%, and these women had more complications such as primary taxicosis and preeclampsia. St. aureus was detected in 16.7% of women in group 1, in 3.3% of women in group 2. Despite the treatment, women diagnosed with this bacterium caused more urinary tract pathologies than other pathogens. In rare cases, Enterobacter aureus, Candida, Str.pyogenes, Proteus mirabilis and St.saprophyticus were detected.We studied the bacteriuria of women's husbands' urine and the level of sperm sterility in order to determine the relationship between the infection of women's sexual partners in the occurrence of urinary tract infections in women. Only husbands of women in group 1 were examined. We paid special attention to the fact that the women involved in our research had only one sexual partner (according to the pregnant woman and her husband). Husbands of 30 women in group 1 submitted urine for bacteriuria, and 12 of them submitted sperm fluid for bacteriological culture. According to the analysis of the results: bacteria were not detected in the urine of 4 (13.3%) men and in the seminal fluid of 1 (8.3%) man. 1ml 1x102 KOE 2 (6.7%), 1x103 4 (13.3%), 1x104 9(30%), 5x104 1(3.3%) were found in men. 1 ml 1x105 KOE 7(23.3%) and 1ml 1x106 KOE 3(10%) were the amounts detected in the urinalysis of men that we considered significant. It should be noted that 2 men with 1 ml 1x106 KOE had chronic pyelonephritis, 1 man had glomerulonephritis, and 1 man with 1 ml 1x105 KOE had chronic cystitis, 1 man had a single kidney. The leukocytes of the same men were high when the semen analysis was performed, 1x105 and 1x106 KOE lig was observed in 1 ml.According to the results of the detection of bacteria in bacteriuria and sperm fluid, bacteria were not detected in the urine of 4 (13.3%) men and in the sperm fluid of 1 (8.3%) man. The name of the type of bacteria was not mentioned in the urinalysis of 5 (16.7%) men with a low amount of bacteria in the urine. Compared to women, E.coli was found in less amount in urine and sperm in men, in 2(6.7%), 1(3.3%), respectively. The most frequently occurring bacteria are St. aureus 6(20%), 4(13.3%) individuals, Klebsiella pneumonia 3(10%), 5(16.7%) individuals, Enterococcus spp. 4(13.3%), observed in 2 (6.7%) people. Other bacteria were detected in rare cases, among which Enterobacter aureus, Candida, Str. pyogenes from 3.3%. From this analysis, it was found that the pathogen found in urine is also present in pathological concentration in semen.Antibacterial therapy was given to men depending on the group in which the most sensitivity was determined. These drugs were prescribed fosfomycin powder 1 time, azithromycin 500 mg once for 3 days, ciprox twice for 5 days. Fosfomycin was prescribed to 2 men, azithromycin to 6 men, Ciprox to 8 men.During pregnancy, only women in the control group did not have any urinary tract pathologies. One (3.3%) woman in group 1 had a congenital single kidney and was treated with her husband for asymptomatic bacteriuria, and she had no pregnancy and delivery complications. At full term, the pregnancy was terminated by cesarean section. Despite the treatment of asymptomatic bacteriuria in the first trimester of pregnancy, several complications occurred in women of groups 1 and 2. Cystitis was the most common pathology, 1 (3.3%) in group 1 and 3 (10%) in group 2. All other diseases occurred in group 2. Among them, gestational pyelonephritis-1(3.3%), prelithiasis-1(3.3%) and hydronephrosis were observed in 2(6.7%) women. The above-mentioned changes were confirmed in US examination and general analysis of urine.When babies were evaluated by Apgar scale, 28(93.3%), 20(76.9%) and 24(100%) babies were born with satisfactory condition, respectively. In group 1, 1 baby was born at 4-5 points and another at 6-7 points. 3 children in group 2 were treated in intensive care with immature and severe asphyxia. 3 (11.5%) babies in this group were born with 6-7 points, 2 of them had neonatal loss. Both of these children were born at full term. Only one mother had chorioamnionitis and was delivered operatively due to ineffective labor induction. The mother of another baby had pre-eclampsia and had an operative delivery.
5. Conclusions
E.coli was found in less quantity in men's urine and sperm than in women. According to the frequency of occurrence, St.aureus is the most common in 6(20%), 4(13.3%) individuals, Klebsiella pneumonia in 3(10%), 5(16.7%) individuals, Enterococcus spp. 4(13.3%), 2 (6.7%) was observed. The causative agent found in urine was also in pathological concentration in the seminal fluid, and the female urine of these men had high KOE. Complications in women whose husbands were not treated may not have developed as a result of asymptomatic bacteriuria, but it is more likely to have aggravated complications. Complications were also more serious in women of the second group. Especially the woman and the unborn child's father, who were not examined and treated, as a result of the repeated transmission of the infection from the man to the woman, proved that women alone are not enough treated.
References
| [1] | Matrizayeva Q.M., Yusupova M.A. “ Assymptom Bacteriuria in Pregnant Women:Obstetric and Perinatal Aspects”. RESEARCH JOURNAL OF TRAUMA AND DISABILITY STUDIES. Oct-2022 ISSN:2720-6866. 167- 171. http://journals.academiczone.net/index.php/rjtds. |
| [2] | Matrizayeva G.D, Ikramova X.S, Saporbayeva I.R. Определить эффективность применения прегравидарной подготовки пациенток с гиперандрогенией для снижения частоты акушерских и перинатальных осложнений// Biologiya va tibbiyot muammolari. -2021, №1. 1 (126), 2021 -yil. 10.38096/2181-5674.2021.1.1. |
| [3] | Hassan H. Infertility profile, psychological ramifications and reproductive tract infection among infertile women, in northern Upper Egypt. Journal of Nursing Education and Practice. 2016; 6(4): 92-108. https://doi.org/10.5430/jnep.v6n4p92. |
| [4] | Оценка опыта применения комбинированного растительного препарата у беременных (многоцентровое ретроспективное наблюдательное исследование) / В. Н. Серов [и др.] // Акушерство и гинекология. – 2013. – № 9. – С. 105-112. |
| [5] | Палагин И.С., Сухорукова М.В., Дехнич А.В., Эйдельштейн М.В., Перепанова Т.С., и др. Антибиотикорезистентность возбудителей внебольничных инфекций мо-чевых путей в России: результаты многоцентрового исследования «ДАРМИС-2018». // Клиническая микробиология и антимикробная химиотерапия. - 2019. - Т. 21, №. 2. - С. 134-146. https://doi.org/10.36488/cmac.2019.2.134-146. |
| [6] | Hassan H. Evidence-Based Practice in Midwifery and Maternity Nursing for Excellent Quality of Care Outcomes. American Journal of Nursing Research, 2020; 8(6): 606-607. doi: 10.12691/ajnr-8-6-3. |
| [7] | Farg D. and Hassan H. Study Hyperemesis Graviderum Requiring Hospital Admission during Pregnancy: Effect of Nursing Implication on Its Progress. American Journal of Nursing Research, 2019; 7(3): 328-341. doi: 10.12691/ajnr-7-3-14. |
| [8] | Никонов А. П. Инфекция мочевыводящих путей и беременность. Практические рекомендации по диагностике и антимикробной терапии / А. П. Никонов, О. Р. Асцатурова // Фарматека. – 2013. – № 12. – С. 50-53. |
| [9] | Новые подходы к диагностике инфекционно-воспалительных заболеваний мочевыводящих путей в период беременности / Н. А. Ломова [и др.] // Эффективная фармакотерапия. – 2013. – № 1. – С. 29-34. |
| [10] | Икрамова Х.С., Абдурахманова Д.Н Матризаева Г.Д. Кровотечение в виде осложнения у обследуемой группе беременных с преэклампсией. International Scientific Review of the Problems and Prospects of Modern Science and Education // International Scientific Review № 1 (32) / XXX International Science Conference (New York. USA, 21-22 January, 2017) P. 79-82. |
| [11] | Отеки у беременных: заболевание или норма? / В. Е. Радзинский [и др.] // Гинекология. – 2014. – Т.16, № 3. – С. 72-74. |
| [12] | Perez-Moreno MO, Pico-Plana E, Grande-Armas J.Group B streptococcal bacteriuria during pregnancy as a risk factor for maternal intrapartum colonization: a prospective cohort study. Med Microbiol. 2017; 66(4): 454–460. DOI: 10.1099/jmm.0.000465. |
| [13] | Mohamed W., Hassan H. Educational Program to Enhance Pregnant Women's Knowledge about Dental Care and Periodontitis Outcomes. ARC Journal of Nursing and Healthcare, 2019; 5(3): 23-33. doi: http://dx.doi.org/10.20431/2455-4324.0503004. |
| [14] | Hassan H., Sobhy S., Rakha E., El-Khayat I. Traditional Practices among Rural Women to Relieve Their Common Pregnancy Minor Discomforts: A Descriptive Study. Medical Science & Healthcare Practice, 2019; 3(2): 56-90. doi:10.22158/mshp.v3n2p56. |
| [15] | Оценка опыта применения комбинированного растительного лекарственного препарата у беременных: многоцентровое ретроспективное наблюдательное исследование / В. Н. Серов [и др.] // Акушерство и гинекология. – 2013. – № 9. – С. 105-112. |
| [16] | Moore A., Doull M., Grad R., Groulx S., Pottie K., et al. Recommendations on screening for asymptomatic bacteriuria in pregnancy. // Canadian Medical Association Journal. -2018. - V.190. - №.27. -P. 823-830. https://doi.org/10.1503/cmaj.171325. |
| [17] | Mukherjee A., Mukherjee A. Urinary tract infection in pregnancy. // Journal of Evolution of Medical and Dental Sciences. - 2018. - V. 7, №. 39. - P. 5113-5118. https://doi.org/10.14260/jemds/2018/961. |
| [18] | Farg D. and Hassan H. Obstetric Outcomes for Teenage and Adult Pregnancy: A Comparative Study. Nursing & Care Open Access Journal, 2020; 7(1): 1-10. doi:10.15406/ncoaj.2020.07.00208. |
| [19] | Hassan H. Fetal and neonatal complications of pregnancy induced hypertension. American Research Journal of Public Health, 2020; 3(1): 1-3. DOI: 10.21694/2639-3042.20003. |
| [20] | Оценка эффективности озонотерапии в комплексном лечении острого гестационного пиелонефрита / М. Р. Гаитова [и др.] // Уральский медицинский журнал. – 2013. – № 9. – С. 76-78. |
| [21] | Перепанова Т.С. Федеральные клинические рекомендации «Антимикробная терапия и профилактика инфекций почек, мочевыводящих путей и мужских половых органов - 2015 г.». // Терапевтический архив. - 2016. - Т.88(4). - С. 100-104. https://doi.org/10.17116/terarkh2016884100-10424. |
| [22] | Hassan H. Self-Care Practices for Women with Gestational Diabetes. EC Nursing and Healthcare, 2020; 2(12): 168-175. |
| [23] | Hassan H. The Impact of Evidence-Based Nursing as The Foundation for Professional Maternity Nursing Practices. Open Access Journal of Reproductive System and Sexual Disorder, 2019; 2(2): 195-197. OAJRSD.MS.ID.000135. DOI: 10.32474/OAJRSD.2019.02.000135. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML