-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(7): 1728-1731
doi:10.5923/j.ajmms.20241407.02
Received: Jun. 8, 2024; Accepted: Jun. 30, 2024; Published: Jul. 2, 2024

Association of Allelic and Genotypic Variants of a Polymorphic Locus T58C Gene SOD 2 Gene in Formation Cardiovascular Form of Diabetic Autonomic Neuropathy in Patients
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSadikova N. G.1, Najmutdinova D. K.1, Boboev K. T.2
1Tashkent Medical Academy, Uzbekistan
2Republican Specialized Scientific and Practical Medical Center of Hematology, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Diabetic autonomic neuropathy (DAN) is the second most common form of damage to the nervous system in diabetes mellitus as a result of disorders of the central and/or peripheral parts of the autonomic nervous system. On average, its incidence is about 40%, and with an increase in the experience of diabetes mellitus for more than 10 years – 60% or more. Diabetic autonomic neuropathy is characterized by polysyndromic clinical manifestations. In this regard, there are a number of forms of diabetic autonomic neuropathy, both in the form of isolated dysfunction of organs and systems, and with their combined lesion.
Keywords: Organs and systems, Vascular and metabolic, Risk factors
Cite this paper: Sadikova N. G., Najmutdinova D. K., Boboev K. T., Association of Allelic and Genotypic Variants of a Polymorphic Locus T58C Gene SOD 2 Gene in Formation Cardiovascular Form of Diabetic Autonomic Neuropathy in Patients, American Journal of Medicine and Medical Sciences, Vol. 14 No. 7, 2024, pp. 1728-1731. doi: 10.5923/j.ajmms.20241407.02.
1. Introduction
- Vascular and metabolic changes common to the development of diabetic polyneuropathy play an important role in the pathogenesis of autonomic neuropathy. The most significant risk factors for the development of diabetic autonomic neuropathy are the patient's age, the duration of diabetes mellitus, and a higher average HbA1c. Diabetic autonomic cardiovascular neuropathy, when clinical symptoms appear, not only dramatically reduces the quality of life, leading to disability, but in some cases is the direct cause of death in patients with diabetes mellitus. It has been proven that cardiovascular autonomic neuropathy is associated with a high risk of arrhythmia and the development of sudden death syndrome [5]. The detection of signs of autonomic dysfunction at the preclinical stage makes it possible to slow down the further progression of autonomic disorders. Another variant of diabetic neuropathy is autonomic neuropathy (AN). Neurological autonomic dysfunction can occur in most body systems, manifesting itself in the form of gastroparesis, constipation, diarrhea, anhidrosis, bladder dysfunction, erectile dysfunction, exercise intolerance, resting tachycardia, pain-free ischemia. The cardiovascular form of diabetic autonomic neuropathy (DAN CF) is damage to nerve fibers that innervate the heart and blood vessels, which often causes severe arrhythmias, determines the formation of pathology of the cardiovascular system (CVS), pain-free ischemia of the heart, complicating the course of DM and leading to death from cardiovascular catastrophes. Pathological HRV assessment tests were found in 7% of patients with newly diagnosed DM type 1 and DM type 2. [1]. The conducted studies indicate an annual increase in the prevalence of DAN CF in patients with DM type 2 to 6% and in patients with DM type 1 to 2%, respectively. In 1998, the Diabetes Control and Complications Trial (DCCT) research group observed 1,441 DM type 1 patients and demonstrated a decrease in heart rate variability (HRV) in 6.2% of the subjects, while Kennedy W. et al. A decrease in HRV was observed during deep breathing and the Valsalva test in 90% and 88% of patients, respectively. Ziegler D. et al. A large cohort of patients with DM type 1 and DM type 2 were studied in 22 medical centers in Austria, Germany, and Switzerland. Pathological results of heart rate variability (HRV) tests were obtained in 25.3% of patients with DM type 1 and in 34.3% of patients with DM type 2 [10]. The prevalence of left ventricular diastolic dysfunction in patients with DM 2 reaches 30-60%. Despite the high prevalence and such a serious prognosis, practitioners know quite little about cardiovascular disorders in DAN CF. According to the epidemiological study by A.L. Vertkin, O.N. Tkacheva, the prevalence of DAN in inpatient patients with DM type 1 and DM type 2 in. Moscow accounted for 47.6%: at the subclinical stage – 28%, and at the clinical stage – 19.6%. At the same time, CF DAN was indicated in the diagnosis in only 2.7% of the total number of patients with this DM complication. The detection of CF DAN in patients is important because CF DAN is associated with increased mortality, cardiovascular disease, chronic kidney disease, perioperative mortality and complications of the lower extremities. Intensive multifactorial intervention aimed at lifestyle changes, intensive glycemic control and reduction of glycemic variability, reduction of CVD risk factors prevents and slows down the progression of CV DAN.It is known that the pathogenesis of DAN is multifactorial and metabolic, antioxidant and vascular disorders are a necessary condition for the formation of this pathology in patients with DM, but the speed of development also depends on genetic predisposition.Polymorphic locus T58C of the SAD2 antioxidant defense gene is located in exon 3 of chromosome 6 (6q25.3), characterized by the replacement of the thymine nucleotide at position 58 with cytosine. This nucleotide substitution leads to a change in the amino acid isoleucine to threonine in the synthesized enzyme SOD2 and contributes to a significant decrease in its activity [3,4,8].The purpose of this study was to study the role of polymorphism of the T58C gene of the SOD2 gene in the development of the cardiovascular form of DM type 2.
2. Materials and Methods
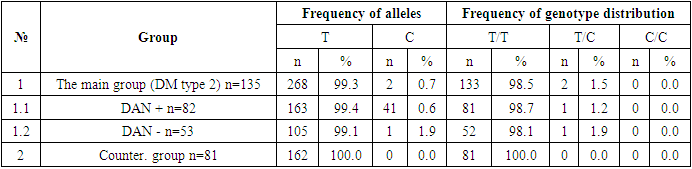
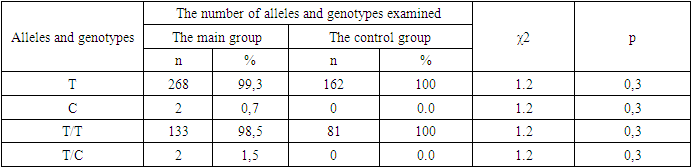
- The study included 135 DM type 2 patients at an average age of 56.3±2.3 years with a disease duration of 5.6± 1.2 years who received outpatient treatment in 3 clinics of the Tashkent Medical Academy. Of these, 69 women at an average age of 52.3±3.4 years and 66 men at an average age of 54.3±2.6 years. The control group consisted of 81 people with an average age of 53.6 ± 2.4 years. All patients were tested for fasting blood sugar and blood sugar after eating 2 hours later, as well as glycated hemoglobin. As a hypoglycemic drug, 88 patients received both DPP - 4 and biguanides, and 47 patients received combination therapy with basal insulin. To identify diabetic autonomic neuropathy of the cardiovascular form (DAN CVF) in DM type 2 patients, all patients underwent Holter monitoring. According to the results of the Holter monitoring parameters, they were divided into 2 groups with DON KVA (+ ) and DAN KVF (-).The results of the study. In patients with DM type 2, the fasting blood glucose level was 7.6±2.3 mmol/l, 2 hours after eating 9.6±1.4 mmol/l. Glycated hemoglobin was on average 9.2 ±1.2%. According to the results of Holter monitoring and standard cardiovascular tests, 82 patients (60.7%) were diagnosed with DAN KVF (+) and 53 patients ((39.2%) DAN KVF (-). To test the role of the T58C polymorphism of the SOD 2 gene in the etiopathogenesis of cardiovascular DAN (CF) in DM type 2 patients, we conducted a comparative associative study in a sample of patients and conditionally healthy individuals of Uzbek nationality.The analysis of associations of the polymorphic locus T58C of the SOD2 gene with the formation of the cardiovascular form of DAN in DM 2 patients was carried out by comparing two samples using the «case-control» platform. The "case" sample was formed from 216 DM2 patients with (n=82) without (n=53) cardiovascular DAN. The control group consisted of 81 conditionally healthy donors of Uzbek nationality (control n=81).The results obtained are shown in Tables 1, 2 and Figure 1.
|
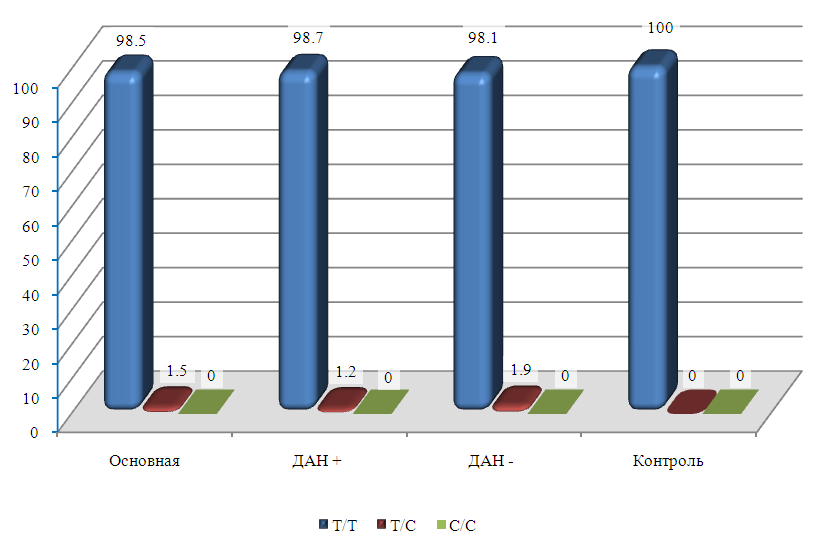 | Figure 1. The frequency of distribution of the T58C polymorphism genotypes of the SOD2 gene in groups of patients with and without DM2 cardiovascular DAN and control |
|
3. Results and Discussions
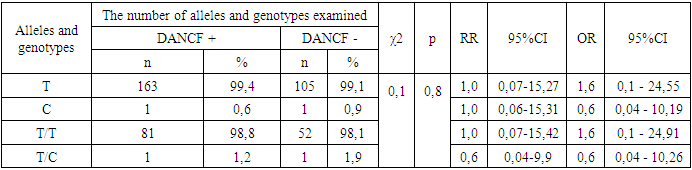
- It should be noted that in this part of the work, there was no clear relationship between the polymorphism of the T58C SOD2 gene and the development of the cardiovascular form of DAN in DM type 2 patients. Allelic variants of this locus within the studied subgroups of patients with and without cardiovascular manifestations were distributed evenly. As can be seen from the table, in the subgroup of patients with the cardiovascular form of DAN, the frequency of the mutational allele C was slightly lower than in the subgroup without DANCF - (0.6% vs. 0.9%, respectively, at χ2=0.1 и р=0.8). The relative risk of the formation of the cardiovascular form of DAN was also below OR=0.6 with a confidence interval of 95%CI: 0.04 – 10.19. When comparing the frequencies of genotypes, the revealed differences were not statistically significant and did not even allow us to detect trends towards differences in their distribution (p>0.05).In a subgroup of patients with cardiovascular syndrome, there was a tendency to decrease the frequency of the T/S genotype compared with patients with DM2 without the cardiovascular form of DAN (1.2% vs. 1.9%, respectively, at -2=0.1 and p=0.8).Thus, a functionally unfavorable allele may not play a significant independent role in the pathogenesis of the cardiovascular form in patients with DM type 2 DAN and is not a significant prognostic marker in our population. Unfortunately, there is no data in the literature on the association of this polymorphism with DAN in patients with DM type 2, which does not allow us to fully interpret the data we have obtained. It is also not possible to conduct a comparative analysis with other ethnic groups. However, it should be emphasized that insignificant differences in statistical processing in comparative samples are undoubtedly related to the low frequency of the mutational allele with a more effective antioxidant protection system. Therefore, it cannot be excluded that this polymorphic locus of the SOD2 gene has a functional significance and is linked to another functionally important polymorphic marker of this gene. As is known, with a low frequency of a certain allele in comparative groups, significant differences, i.e., a significant effect can be detected only with a large sample size of more than 1000-2000 individuals.
4. Conclusions
- In the development of diabetic autonomic neuropathy of the cardiovascular form, the unfavorable allele of the T58C polymorphism of the SOD2 gene does not play a significant role and is not a prognostic marker in patients with type 2 diabetes mellitus in our population. However, insignificant differences in statistical processing in comparative samples are associated with a low frequency of the mutation allele with a more effective antioxidant protection system.
References
| [1] | Dedov I.I., Peterkova V.A., Bolotskaya L.L., etc. Complications of type 1 diabetes mellitus and ways to solve the problem. Diabetes mellitus. 1999; 3: 2–6. [Dedov I.I., Peterkova V.A., Bolotskaya L.L. et al. Complications of type 1 diabetes mellitus and remedies. Diabetes Mellitus. 1999; 3: 2–6. (in Russian)] |
| [2] | Balcıoğlu AS, Müderrisoğlu H. Diabetes and cardiac autonomic neuropathy: Clinical manifestations, cardiovascular consequences, diagnosis and treat ment. Diabetes Care. 2010 Feb; 33(2): 434-41. |
| [3] | Fernandes RC, Hasan M, Gupta H, Geetha K, Rai PS, Hande MH, D'Souza SC, Adhikari P, Brand A, Satyamoorthy K. Host genetic variations in glutathione-S-transferases, superoxide dismutases and catalase genes influence susceptibility to malaria infection in an Indian population. Mol Genet Genomics. 2015 Jun; 290(3): 1155-68. doi: 10.1007/s00438-014-0984-4. Epub 2015 Jan 9. PMID: 25573779. |
| [4] | Işikli A, Kubat-Üzüm A, Satman İ, Matur Z, Öge AE, Küçükali Cİ, Tüzün E, Erden S, Özkök E. A SOD2 Polymorphism is Associated with Abnormal Quantitative Sensory Testing in Type 2 Diabetic Patients. Noro Psikiyatr Ars. 2018 Apr 20; 55(3): 276-279. doi: 10.29399/npa.23027. PMID: 30224876; PMCID: PMC6138222. |
| [5] | Maser R, Lenhard M, DeCherney G. Cardiovascular autonomic neuropathy: the clinical significance of its determination. Endocrinologist. 2000 Jan; 10: 27-33. |
| [6] | Mogensen U. M., Jensen T., Køber L.et al., “Cardiovascular autonomic neuropathy and subclinical cardiovascular disease in normoalbuminuric type 1 diabetic patients,” Diabetes, vol. 61, no. 7, pp. 1822–1830, 2012. |
| [7] | Spallone V., Ziegler D., Freeman R.et al., “Cardiovascular autonomic neuropathy in diabetes: clinical impact, assessment, diagnosis, and management,” Diabetes Metabolism Research and Reviews, vol. 27, no. 7, pp. 639–653, 2011. |
| [8] | Taş A, Sılığ Y, Pinarbaşi H, GüRelık M. Role of SOD2 Ala16Val polymorphism in primary brain tumors. Biomed Rep. 2019 Mar; 10(3): 189-194. doi: 10.3892/br.2019.1192. Epub 2019 Feb 7. PMID: 30906548; PMCID: PMC6403480. |
| [9] | Vinik A.I., Erbas T. Recognizing and treating diabetic autonomic neuropathy. Cleve Clin. J. Med. 2001; 68(11): 928–30, 932, 934–44. DOI: 10.3949/ccjm.68.11.928. |
| [10] | Ziegler D., “Diabetic cardiovascular autonomic neuropathy: Prognosis, diagnosis and treatment,” Diabetes Metabolism Reviews, vol. 10, no. 4, pp. 339–383, 1994. |