-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(6): 1699-1703
doi:10.5923/j.ajmms.20241406.49
Received: Jun. 6, 2024; Accepted: Jun. 25, 2024; Published: Jun. 26, 2024

Histochemical Aspects of Pathway Anomalies in Tetralogy of Fallot
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNizamov Kh. Sh., Eshbaev E. A., Allaberganov D. Sh., Nizamova N. G., Allanazarov I. M.
Samarkand State Medical University & Tashkent Medical Academy, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

It is important to understand the topographic-histological nature of the conduction tracts in the heart in Tetralogy of Fallot, to confirm the presence of a hypoplastic process in the malformations of the conduction tracts and to clarify their morphological aspects. When stained with silver, most tracts are brown-black, reticular fibers and elastic fibers are golden, and collagen fibers and other tissue branches are brown. In the Tetralogy of Fallot, varying degrees of changes are noted, quantitative and qualitative changes in the bundles extending from the sinoatrial node, hypertrophic and atrophic changes in different branches of the ventricles of the heart. In particular, with defects of the subvalvular foramen, most of the fibers arising from the Hiss nucleus branch into the right ventricle, and a small number of fibers into the left ventricle.
Keywords: Tetralogy of Fallot, Morphology, Conduction pathways, Histochemical method
Cite this paper: Nizamov Kh. Sh., Eshbaev E. A., Allaberganov D. Sh., Nizamova N. G., Allanazarov I. M., Histochemical Aspects of Pathway Anomalies in Tetralogy of Fallot, American Journal of Medicine and Medical Sciences, Vol. 14 No. 6, 2024, pp. 1699-1703. doi: 10.5923/j.ajmms.20241406.49.
Article Outline
1. Introduction
- The relevance of the problem lies in the fact that the incidence of Tetralogy of Fallot in the Republic of Uzbekistan is 1.4 times higher than in other countries of the world, and 1.1 times higher than in the countries of Central Asia. This is explained by the increase in the demographic index of the population. On the other hand, this is due to the increase in marriages between relatives. However, due to the lack of full screening in the early stages of pregnancy and failure to follow recommendations for termination of pregnancy in cases of detected congenital heart defects, these pathologies are growing at different levels. According to the RCPA, the incidence rate of Tetralogy of Fallot per 1000 births during 2022 will be 23-27 cases. Of course, this data analysis is presented with a specific patient index. As a result of identifying Tetralogy of Fallot during pregnancy screening in the USA and European countries and the unconditional implementation of practical recommendations for terminating pregnancy using this method, the morphological substrates of the processes of morphological adaptation in heart tissue were identified. in the postnatal period show that the morphological substrates of the processes of cardiac tissue are not fully understood. Although information about the morphological adaptation of the Tetralogy of Fallot has been replenished as a result of various scientific studies in most of the territory of the Russian Federation and foreign countries, complete information about the changes that have occurred under the influence of social and regional-geographical factors has not been obtained.
2. Research Aim
- The aim of this research is to investigate the pathomorphology of conduction pathways in cases of sudden cardiac death associated with Tetralogy of Fallot in congenital heart disease.
3. Materials and Methods
- Heart tissue from autopsies of 56 children under 1 year of age who died of congenital heart defects at the Republican Center of Pathological Anatomy and the National Children's Center. Sections of heart tissue taken by morphologic method were frozen in 10% buffered formalin for 72 hours. Then, after washing in running water for 1 hour, they are dehydrated in ascending grade alcohols (70,80,90,100%). The slices are then frozen in paraffin and poured into cassettes. Using a microtome, 5-7 µm thick slices are taken, deparaffinized in xylene and stained with hematoxylin and eosin. The obtained results are viewed under a light microscope, microphotographs are made and morphometrically analyzed. The method of silver impregnation revealed that predominantly conducting networks in myocardium, including the conducting pathway of Hiss nucleus and branches departing from it, Purkinje fibers are stained in brownish-black color.
4. Results and Discussions
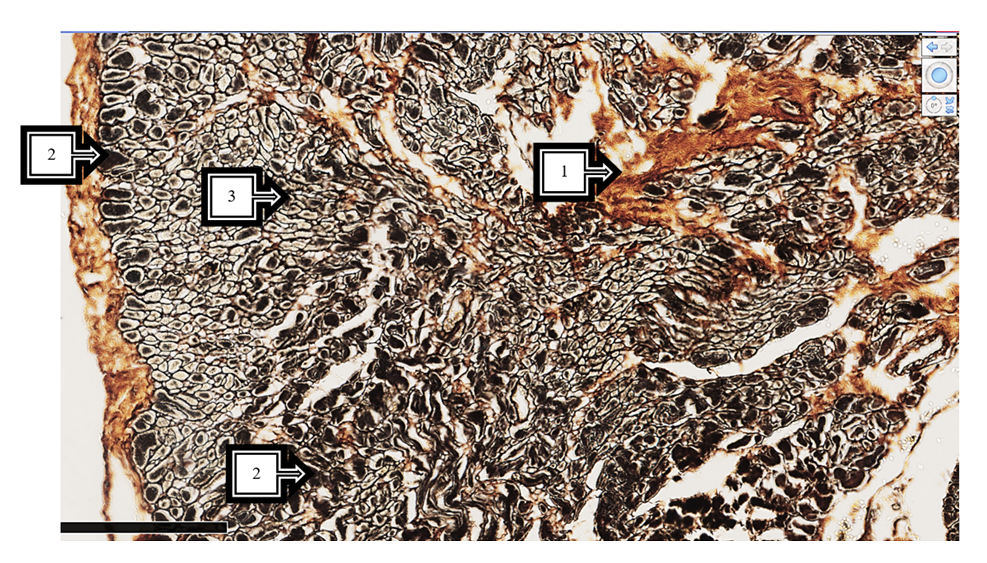
- In an interventricular septal defect of Tetralogy of Fallot, hemodynamic disturbances result in right ventricular hypertrophy from a physiological point of view, but a large number of conducting fibers from the right stem of Purkinje fibers are found between these muscle bundles.Preservation of subendocardial edema, dense reticular structures around the conducting fibers, and between the bundles of typical cardiomyocytes various branched foci of sparse fibrous connective tissue of golden-yellow color (on silver impregnation) are determined. This is characterized by causing congestion of the conductive pathways (see Figure 1). In most cases, the perimeter of clearly formed interstitial swellings between the endocardium and myocardium is clearly depicted on silver impregnation staining, and this process is one of the morphologic substrates confirming the loss of myocardial automaticity.
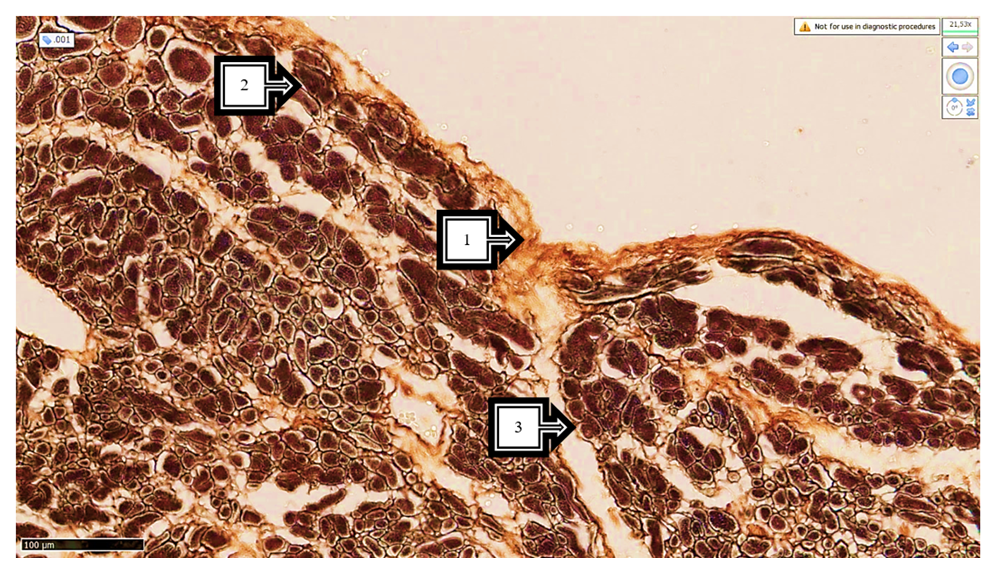 | Figure 1. Subvalvular branch of the right ventricle in Tetralogy of Fallot. Endocardial elastofibrosis (1), atypical clusters of cardiomyocytes of different sizes (2), edema and sclerotic foci in interstitial tissue (3). Stain: Silver impregnation. Size 10x10 |
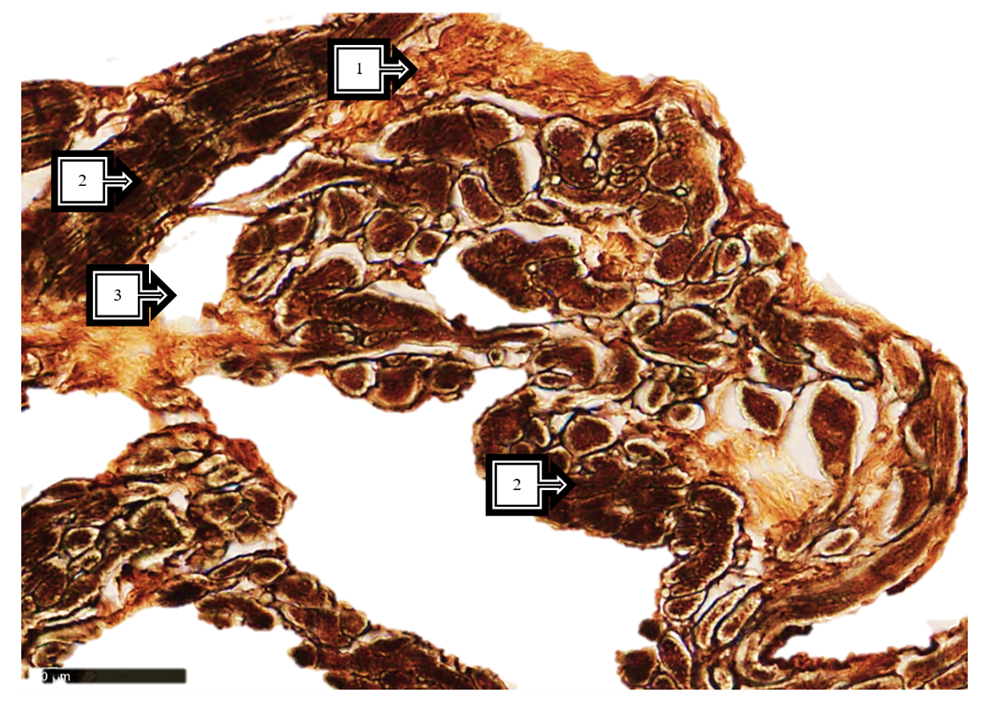 | Figure 2. Tissue of the right ventricle and subarachnoid region of the left ventricle in Tetralogy of Fallot. Endocardium with elastofibrosis of different thickness (1), atypical cardiomyocytes with different bundle sizes (2), interstitial ballooning and foci of destruction (3). Stain: Silver impregnation. Size 10x10 |
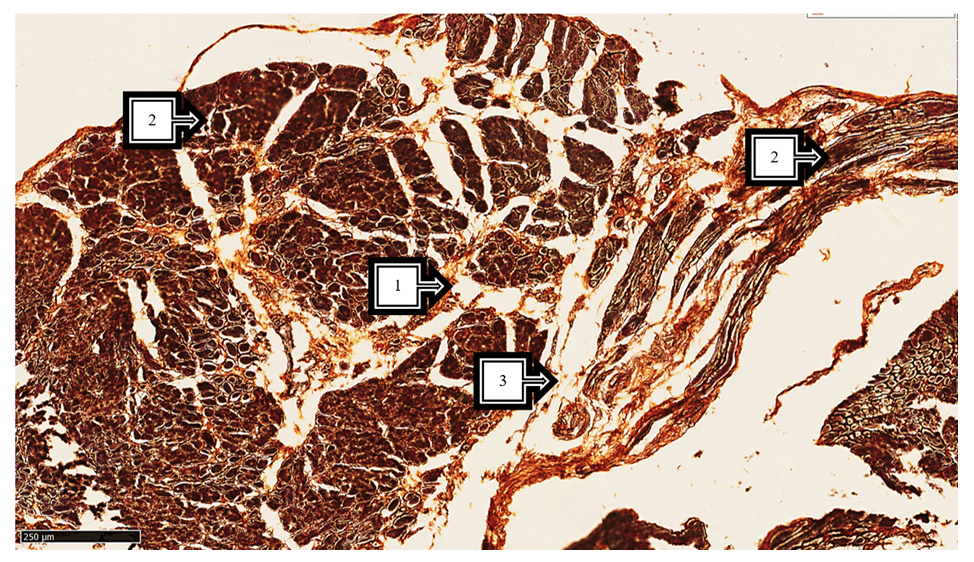 | Figure 3. In Tetralogy of Fallot, tissue is taken from the subatrial region of the right and left ventricle. Scar foci around Hiss bundles (1), between foci of sclerosis (2), preserved bundles of atypical cardiomyocytes of different sizes (2), foci of interstitial edema and destruction (3). Dye: Silver impregnation. Size 10x10 |
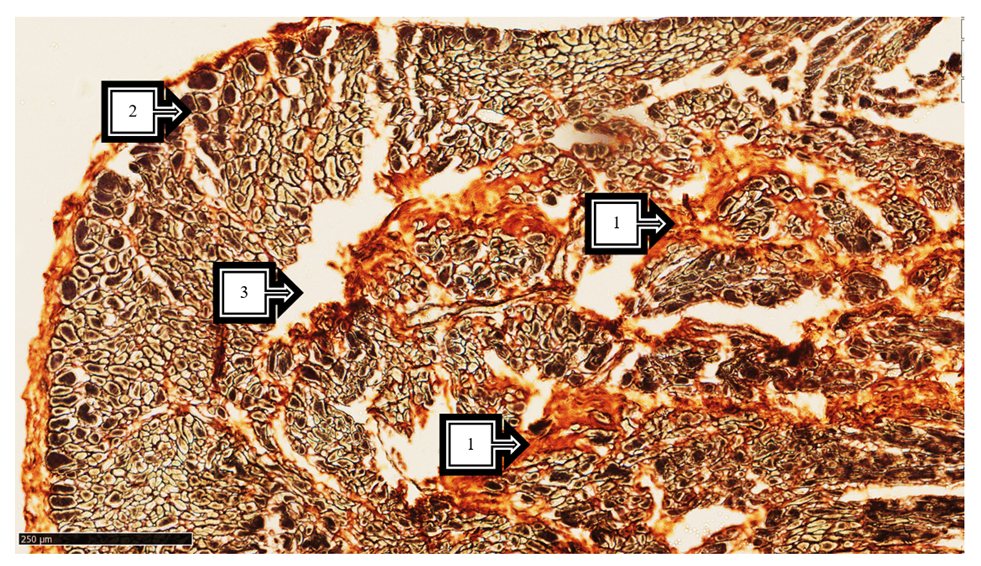 | Figure 4. Tissue taken from the right ventricle-pulmonary trunk transition site in Tetralogy of Fallot. Massive disorganized golden collagen fibers (1), atypical cardiomyocytes of different sizes (2), alternating edema and foci of destruction (3). Stain: Silver impregnation. Size 10x10 |
 | Figure 5. Tissue of the pulmonary trunk of the right ventricular branch in Tetralogy of Fallot. Gold-colored collagen fibers (1), atypical cardiomyocytes of various sizes (2), interstitial ballooning and foci of destruction (3). Stain: Silver impregnation. Size 10x10 |
5. Conclusions
- In conclusion, depending on the localization of the developmental anomaly in Tetralogy of Fallot, hypoplasia of the development of the common conductive pathways of the heart was detected, precisely at the borders and perimeter of the malformation. In hypoplasia of silver impregnation, the presence of conducting fibers with bright cytoplasm of small, thin fibers and hypertrophic changes of Purkinje fibers in the elastic branch of the subendocardial branch muscle was revealed. It was found that this paradox consisted in the accumulation of impulses in the undeveloped field of atypical cardiomyocytes and their passage through the formed atypical myocytes in the form of hyperimpulse with a parallel increase of typical and atypical cardiomyocytes in this field. Muscle bundles of different sizes and irregular collagen fiber centers formed by coarse fibers are precisely defined around the defect. This, in turn, blocks the synchronous conduction of impulses in the morphologically adapted myocardium, leading to the rapid onset of clinical and morphological cardiac fibrillation and acute cardiac death. Consideration of this phenomenon in the field of practical cardiac surgery forms the morphological basis for the possibility of palliative choice of treatment tactics and practice of radical correction.