-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(6): 1606-1611
doi:10.5923/j.ajmms.20241406.28
Received: May 5, 2024; Accepted: Jun. 3, 2024; Published: Jun. 19, 2024

Clinical Characteristics of Autonomic Support of the Body in Acute Pneumonia in Young Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbdurakhmanov Jasur Nematovich, Sharipova Oliya Askarovna, Bakhronov Sherzod Samievich, Mamatkulova Dilrabo Khamidovna
Samarkand State Medical University, Samarkand, Uzbekistan
Correspondence to: Bakhronov Sherzod Samievich, Samarkand State Medical University, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

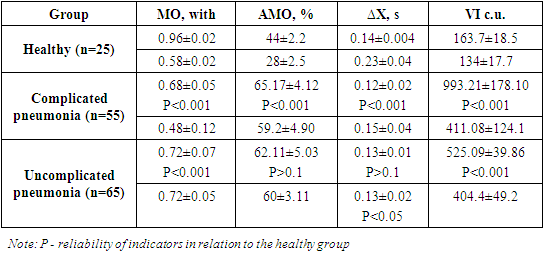
Introduction. Bronchopulmonary diseases in young children, including acute pneumonia, despite significant advances in the study of pathogenesis, clinical manifestations, principles of diagnosis, therapy, and prevention, continue to remain one of the pressing problems in modern pediatrics. Purpose of the study. To study the clinical characteristics of the vegetative support of the body during acute pneumonia in young children. Materials and research methods: 120 children aged from 3 months to 4 years were under observation. The patients were divided into two groups: group I 65 patients with uncomplicated pneumonia, group II 55 patients with complicated pneumonia. The polysegmental form predominated inpatients with complicated pneumonia 22(40%), whereas in patients with uncomplicated pneumonia the focal form predominated 35 (53.8%). Results and its discussion. The results of our study show greater tension of the sympathoadrenal system in complicated pneumonia. This can be seen in the Mo indicators and ∆X, which were sharply reduced in both age groups. In patients with uncomplicated pneumonia, although the indicator Mo and ∆Х were also reduced, but the failure of adaptation mechanisms did not occur, as evidenced bychanges in ∆Х parameters, which were unreliably reduced. Therefore, a reasonable combination of etiotropic pathogenetic therapy with adaptive medicine methods aimed at correcting autonomic imbalance, reactivity and increasing the adaptive capabilities of the body is necessary. Conclusion. Generally, the peculiarities of the functioning of the ANS in complicated and uncomplicated forms of community-acquired pneumonia indicate a disturbance not only of reactivity in the respiratory system, but also of the whole organism. Such a violation of reactivity leads to the fact that not only etiotropic agents, but also perinatal pathology, can cause a deterioration in the child’s condition during the height of the disease.
Keywords: Autonomic nervous system, Pneumonia, Adaptation
Cite this paper: Abdurakhmanov Jasur Nematovich, Sharipova Oliya Askarovna, Bakhronov Sherzod Samievich, Mamatkulova Dilrabo Khamidovna, Clinical Characteristics of Autonomic Support of the Body in Acute Pneumonia in Young Children, American Journal of Medicine and Medical Sciences, Vol. 14 No. 6, 2024, pp. 1606-1611. doi: 10.5923/j.ajmms.20241406.28.
Article Outline
1. Introduction
- Bronchopulmonary diseases in young children, including acute pneumonia, despite significant advances in the study of pathogenesis, clinical manifestations, principles of diagnosis, therapy, and prevention, continue to remain one of the pressing problems in modern pediatrics [9,10,17]. According to WHO, about 155 million cases of pneumonia in children are registered annually worldwide, with approximately 1.4 million deaths occurring before the age of five years [16]. In 2023, pneumonia killed more children than any other infectious disease, killing more than 700,000 children under five each year, or about 2,000 every day [16]. Globally, there are more than 1,400 cases of pneumonia per 100,000 children, or 1 in 71 children each year, with the highest incidence in South Asia (2,500 cases per 100,000 children) and West and Central Africa (1,620 cases per 100,000 children).The prevalence of pneumonia in the general child population according to statistics for Uzbekistan (2015) is 2.91%. A significant role in the development of pneumonia is played by microbial aggression, to which the body is not able to form an adequate response. It is under the influence of nonspecific damaging factors that the body’s adaptive capabilities are reduced, which creates conditions for infection of the lung tissue [1,4,12]. There is no doubt that the state of the autonomic nervous system (ANS) plays a significant role in the occurrence and development of respiratory pathology. One can note the dual participation of the nervous system in the formation and development of inflammation: on the one hand, undoubtedly, the influence of the inflammatory process on the nervous system, on the other hand, the participation of altered reactions of the nervous system in the pathogenesis of inflammation [5,6]. Violations of the ANS function in pneumonia occur secondaryly and are somatically caused. Also, according to Yurkov A. Yu. [19] ANS dysfunction in diseases is associated with a decrease in the body’s vascular supply, high intensity of anabolic processes and changes in the functional state of both of its parts. According to Wayne A.M. [15]. autonomic dysfunction is a syndrome of somatic diseases, including pneumonia.A number of authors have identified dysfunction of the ANS in diseases of the respiratory system in adults and the need for correction of autonomic disorders during their treatment [5,19].Meanwhile, in the literature, information about the state of the autonomic nervous system (ANS) and autonomic regulation of heart rate in older children with acute pneumonia is scarce [6,13,18]. The functional state of the ANS in young children with acute pneumonia has been studied in modern medical literature few, and the results obtained are contradictory. The authors unanimously admit that the problem of ANS disorders in acute pneumonia really exists.When assessing the activity of the ANS, its main indicators should be taken into account: autonomic tone (AT), autonomic reactivity (AR) and autonomic support (AS). AT and AR give an idea of the state of homeostatic equilibrium of the body (HER), and AS - about the functional reserves of the body and the adaptive mechanisms of its formation [6,14]. When identifying ANS dysfunction, its nature and level of damage (segmental, suprasegmental) are taken into account.It has been established that the tension of autonomic regulation in patients depends on the activity and prevalence of the pathological process [11]. Fluctuations in the parameters of ANS dysfunction make it possible to judge not only the course of the disease, but also to predict its outcome. Underestimation of obvious or hidden disorders of the ANS in the clinic makes it difficult to restore disorders, maintains a low quality of life for patients and leads to a decrease in the effectiveness of treatment [3,6]. Successful rehabilitation of patients with acute pneumonia requires an integrated approach involving not only etiotropic drugs in treatment, but also a targeted effect on ANS dysfunction and restoration of the activity of the body’s defense systems [6,8].These arguments are confirmed by cardiointervalographic studies, which allow early diagnosis of autonomic disorders for the development of algorithms for evidence-based methods of correction and prevention, which is of great importance for medical science and healthcare practice.
2. Purpose of the Study
- To study the clinical characteristics of the vegetative support of the body during acute pneumonia in young children.
3. Materials and Research Methods
- 120 children aged from 3 months to 4 years were under observation. All patients with acute pneumonia that we examined were divided into two groups: group I consisted of 65 patients with uncomplicated pneumonia, group II consisted of 55 patients with complicated pneumonia. The control or conditional norm group included 55 healthy children of the same age.When studying age gradation, we found that acute pneumonia was most common in children in the first year of life, so 51.7% of children were aged 3 months or older. Up to 1 year, 28.3% were aged 1 to 2 years and 24% were aged 2 to 4 years. The average age of children under one year was 6.92 ± 0.26 months, for children from 1 to 4 years old it was 1.92 ± 0.08 years. The distribution of patients by gender showed a predominance of boys 73 (60.8%), compared to girls 47 (39.2%).The radiography picture of damage to the respiratory organs was characterized by the presence of focal shadows on both sides in 86 (71.7%) children, the right-sided nature of the pneumonic process occurred in 22 (18.3%) patients and in 12 (10%) patients the lesion had a left-sided nature.The distribution of morphological forms of pneumonia during radiography studies showed a predominance of polysegmental forms inpatients with complicated pneumonia 22(40%),whereas in patients with uncomplicated pneumonia the focal form predominated 35 (53.8%). Lobar and subtotal pneumonia occurred only in patients with a complicated form of pneumonia 8 (14.5%). The focal confluent form of pneumonia was more common in patients with uncomplicated pneumonia, compared with complicated ones: 8(14.5%) and 24(36.9%), respectively.The diagnosis was formulated in accordance with the classification adopted at a meeting of pediatric pulmonologists held as part of the XVIII National Congress on Respiratory Diseases in Yekaterinburg (December 2008). When making a diagnosis, the morphological forms of pneumonia, the nature of complications, the course of the disease, the degree of respiratory failure, the localization of the inflammatory process in the lungs, and the premorbid background were also taken into account.Registration of cardiointervalograms (in the amount of 100 complexes in each case) was carried out on a Kolibri-Carmine cardiointervalograph with subsequent computer processing. The following indicators were calculated and assessed: mode (Mo) - the values of the most frequently occurring values of RR intervals in the series under study, mode amplitude (AMo) - the percentage of values of RR intervals corresponding to the mode; variation range (∆X) – the difference between the maximum and minimum RR intervals. The voltage index (SI) was directly calculated using the formula AMo(%)/(2 MO×∆Х(s)).A general clinical examination of sick children was carried out in the laboratory of the multidisciplinary clinic of Samarkand State Medical University.
4. Results and Its Discussion
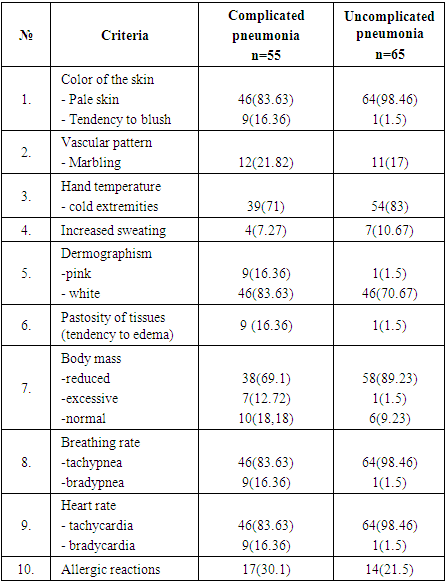
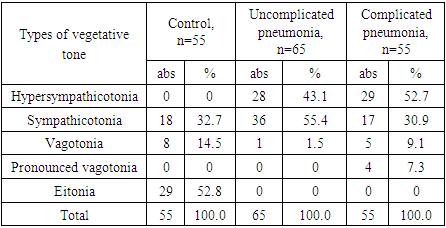
- From the anamnesis it was revealed that the most significant predictors in the development of vegetative visceral dysfunctions in childrenbothgroups of mothers had anemia in 65 (%) and 55 (%) cases, allergic diseases in 27 (49.1%) and 32 (49.2%) and chronic otolaryngology pathology in 23 (41.8%) and 26 (40%) of complicated and uncomplicated pneumonia, respectively.In a detailed study of the anamnesis of the studied children, we identified the manifestation of autonomic disorders in 98 (81.7%) of those studied before 1 year of age, which were characterized by regurgitation in 52 (94.5%) and 51 (78.4%) (respectively complicated and uncomplicated pneumonia), abdominal bloating in 48(87.3%) and 52(80%), restless sleep in 38(69.1%) and 41(63.1%), tendency to constipation 41(74.5%) and 45(69.2%), wakefulness at night in 29(52.7%) and 31(47.7%), as well as colic in newborns in 48(87.3%) and 47(72.3%). In 56(57.1%) children they were observed in various combinations, in 42(42.9%) as one isolated symptom.In general, the functional dysfunctions of the gastrointestinal tract that we identified may be a prestage of the development of vegetative dystonia in pneumonia in children.As is known, the severity of pneumonia is determined by the severity of clinical manifestations and the presence of complications in patients [2,3].The condition of sick children upon admission largely depended on the form of the disease. Thus, 54 (83.1%) sick children with an uncomplicated form of pneumonia had a moderate condition upon admission, while in patients with complicated pneumonia 12 (21.8%) had an extremely severe condition, 43 (78.2%) %) – heavy. Our data show that in young children severe forms of pneumonia predominated, amounting to 55%.As is known, data on what day of illness patients went to the hospital is an important indicator, since the effectiveness of inpatient treatment depends on this [8]. When studying the number of visits to the hospital, we noted that almost half of the visits took place within 4 to 5 days (48.33%). In total, in 24 cases the visit took place on the second and third days of illness (20%). The average rate of hospitalization in patients with complicated pneumonia was 5.62 ± 0.2 days, while in patients with uncomplicated pneumonia 4.3 ± 0.15 days for the entire observed group was 4.9 ± 0.2 days.Considering the important nature of complaints and clinical manifestations in autonomic dysfunctions, we provide their detailed characteristics in patients with acute pneumonia in Table 1; 2.The predominance of vagotonia was evidenced by complaints from the mother about sweating in 33 (60%) and 19 (34.5%) (hereinafter: respectively, in patients with complicated and uncomplicated pneumonia); normal body temperature – in 9 (16.4%) and 1 (1.5%); refusal to eat – in 9 (16.4%) and 1 (1.5%); headaches 6(10.1%) and 1(1.5%); periodic abdominal pain – in 15 (27.3%) and 12 (18.46%); increased drowsiness – in 9 (16.4%) and 1 (1.5%); nausea – in 15 (27.3%) and 12 (18.46%); vomiting – in 32 (58.2%) and 28 (43.1%); diarrhea – in 12 (21.8%) and 11 (17%) patients. These patients had such clinical signs as marbling of the skin - in 12 (21.8%) and 11 (17%); red dermographism – in 9 (16.4%) and 1 (1.5%) patients. A tendency to edema was noted in 9 (16.4%) and 1 (1.5%), excess body weight (paratrophy) - in 7 (12.72%) and 11 (17%), bradypnea - in 9 (16, 4%) and 1 (1.5%) patients, as well as allergic reactions in 17 (31%) and 14 (21.5%) and bradycardia in 9 (16.4%) and 1 (1.5%) examined.
|

|
|
|
5. Conclusions
- Generally, the peculiarities of the functioning of the ANS in complicated and uncomplicated forms of community-acquired pneumonia indicate a disturbance not only of reactivity in the respiratory system, but also of the whole organism. Such a violation of reactivity leads to the fact that not only etiotropic agents, but also perinatal pathology, can cause a deterioration in the child’s condition during the height of the disease. Therefore, a reasonable combination of etiotropic pathogenetic therapy with adaptive medicine methods aimed at correcting autonomic imbalance, reactivity and increasing the adaptive capabilities of the body is necessary.
Conflict of Interest
- The authors declare no conflicts of interest or special funding for the current study.