-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(5): 1192-1196
doi:10.5923/j.ajmms.20241405.10
Received: Feb. 23, 2024; Accepted: Mar. 20, 2024; Published: May 9, 2024

The Use of a Personal Health Card Mobile Application for the Prevention of Cardiovascular Diseases at the Primary Health Care Level
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRasulova Zulfiya Dadaevna, Shayxova Umida Raufovna
Central Consultative and Diagnostic Polyclinic No. 1 of the Main Medical Department under the Administration of the President of the Republic of Uzbekistan, Tashkent, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

To evaluate the use of a personal health card mobile application and the development of an individual wellness program for the prevention of cardiovascular diseases (CVD) at the primary health care level. 279 patients with CVD and previously unobserved with cardiovascular pathology aged 30-70 years were examined, including: standard questionnaire survey; assessment of hemodynamic and anthropometric parameters; ECG; serum assessment of lipid spectrum, glucose, creatinine, urea, uric acid level, C-reactive protein; glomerular filtration rate (GFR) by calculation method according to the formula CKD-EPI; determination of elasticity and biological age of blood vessels (plethysmography), metabolic parameters using bioimpedance analysis of body composition; exercise tolerance (six-minute walk test (SWT), Borg scale for assessing the intensity of shortness of breath, Roufier test, mass test for determining the physical condition of E.A.Pirogov); assessment of quality of life (QOL) and psychosocial factors (stress, social isolation, depression) according to the Reeder L. questionnaire and the EQ-5D health and quality of life assessment questionnaire, EQ–VAS scale. An electronic questionnaire survey card has been developed. They were examined initially and after 3 months of drug and non-drug rehabilitation.
Keywords: Personal health card, Mobile application, Cardiovascular diseases, Cardiovascular risk, Rehabilitation
Cite this paper: Rasulova Zulfiya Dadaevna, Shayxova Umida Raufovna, The Use of a Personal Health Card Mobile Application for the Prevention of Cardiovascular Diseases at the Primary Health Care Level, American Journal of Medicine and Medical Sciences, Vol. 14 No. 5, 2024, pp. 1192-1196. doi: 10.5923/j.ajmms.20241405.10.
Article Outline
1. Intorduction
- Cardiovascular diseases (CVD) continue to be an urgent health problem for most countries of the world [1]. Information technologies are being actively introduced into various spheres of life, including healthcare, which leads to a fundamental change in the quality of people's lives. Cardiological rehabilitation (CR) is recognized as a basic component of primary and secondary cardiovascular prevention and is recommended for both patients with CVD and risk factors (RF) of CVD [2]. Contrary to evidence of a reduction in the risk of sudden death, recurrent coronary events and the progression of atherosclerosis, the positive effect of CR on the socio-psychological status of patients and quality of life, low adherence to its programs is universally stated [2]. The clinical relevance of CR is due to the relationship between the number of physical training sessions (PT) and improved prognosis after a coronary event: every 5 performed PT is associated with lower mortality (adjusted risk ratio (RR) = 0.87 [95% CI: 0.83–0.92]); reduction of the overall risk of cardiac events (adjusted RR = 0.69 [95% CI: 0,65–0,73]) [2,3].The need for healthcare to increase the volume of CR can be realized within the framework of new organizational models integrating its non-stationary forms and the capabilities of telecommunication technologies [2]. The effectiveness of telemedicine cardiorehabilitation (TMCR) is confirmed by the findings of studies demonstrating that in TMCR and traditional CR (based on centers/departments), indicators of physical performance (PPf), quality of life, mortality and cardiac events associated with FT are comparable [8,11].Mobile healthcare (mHealth) is one of the promising, dynamically developing areas of eHealth, the purpose of which is to provide mobile and wireless technologies for information support in the field of healthcare, provision of medical services and ensuring a healthy lifestyle, monitoring the state of clinical and hemodynamic parameters in various CVD [4,5]. The World Health Organization defines it as "medical clinical and public health practices based on mobile device data, including mobile phones, monitors, personal digital assistants and other wireless devices" [7,10,11]. The most active countries in the mHealth sector are primarily those with high per capita income. According to the survey, 72% of doctors in Germany, Great Britain and France actively use mobile technologies in their practice [1,6,9]. The advantages of such technologies are obvious: on the one hand, they are able to make healthcare more accessible, convenient and understandable for the patient, on the other hand, they can provide the doctor with comprehensive technical and advisory support, which ultimately will lead to an improvement in the quality of medical care.The purpose of the study: to evaluate the use of a personal health card mobile application and the development of an individual wellness program for the prevention of CVD at the primary health care level.
2. Material Method
- Research materials and methods. 279 patients with CVD and previously unobserved with cardiovascular pathology aged 30-70 years were examined, including: standard questionnaire survey; assessment of hemodynamic and anthropometric parameters; ECG; serum assessment of lipid spectrum parameters (cholesterol CH, low-density lipoproteins LDL, triglycerides TG, high-density lipoproteins HDL, CH-nonHDL), serum glucose, creatinine, urea, serum uric acid level, C-reactive protein; glomerular filtration rate (GFR) by calculation using the CKD-EPI formula; determination of elasticity and biological age of blood vessels (plethysmography), bioimpedance body composition. The level of exercise tolerance and PPf was determined by the results of the six-minute walk test (SWT), the Borg scale for assessing the intensity of shortness of breath, the Roufier test, the mass physical condition determination test E.A.Pirogov, 1984. The indicators of quality of life (QOL) and psychosocial factors (stress, social isolation, depression) were evaluated using the Reeder L questionnaire and the EQ-5D health and quality of life assessment questionnaire, EQ–VAS scale. An electronic questionnaire survey card and a personalized automated health card have been developed as part of the development of eHealth with the implementation of organizational, clinical, epidemiological, preventive and educational aspects of healthcare through the integrated use of mobile communication devices, application software (mobile applications [1,2].All patients were divided into two groups: the I-st (n=160) main group on the background of drug and non–drug therapy and correction of RF, underwent rehabilitation according to a selected individual program in a group with doctors within the framework of the School of CVD Prevention, the second II - the comparison group (n=107) on the background of drug and non-drug therapy and correction of RF, they independently underwent rehabilitation according to a selected individual rehabilitation program using a mobile application and controlled their indicators independently (weight, body mass index BMI, blood pressure, heart rate). The control group consisted of 22 conditionally healthy individuals. The rehabilitation program included: the development of an individual program for rational nutrition, overweight and obese with a decrease in basal metabolism by 10-30%; a complex of physical rehabilitation; a program for psychological relief. The training of patients in the "School for the Prevention of CVD", including (physical rehabilitation complex) included group gymnastics classes according to the author's scheme 3 times a week for 1 hour, physical therapy with aerobic training, dosed walking depending on FT daily, nutrition training, psychological relief classes that increased motivation for a healthy lifestyle life. They were examined initially and after 3 months of drug and non-drug rehabilitation.Statistical processing of the research results was carried out using a generally accepted method using a personal computer (Excel 2016 program). The arithmetic mean (M) and the error of the arithmetic mean (m) were determined. To determine the statistical significance of the differences between the compared indicators, the Student's t-test was used.
3. Research Results and Discussion
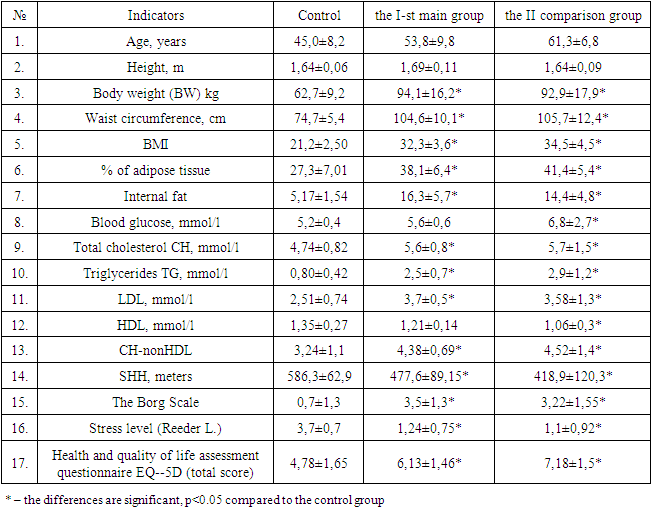
- The creation of an information system in a polyclinic is due to the need to use a large and constantly growing amount of information in solving therapeutic, static and other tasks. The development of information technologies and modern means of communication, the appearance in medical institutions of a large number of automated medical devices, tracking systems and individual computers have led to a new round of interest and to a significant increase in the number of medical information systems, both in large medical centers with large flows of information, and in medium-sized medical centers or in clinical departments [4,6].When filling out an electronic card, patient data, medical history, clinical and laboratory examination data, determination of the level of physical performance are entered, anthropometric and metabolic indicators, health indicators and stress levels are determined, which are entered into the card, CVR is automatically calculated according to SCORE2, risk group, risk factors and target values are determined A rehabilitation program with a scheme of rehabilitation programs was then proposed. An electronic personalized health card and a mobile application based on it have been developed. According to which the CVR according to SCORE2, risk groups, the level of PPf were automatically calculated according to the developed five-step scale based on the results of the SWT test, the Borg scale; stress level, the total indicator of quality of life; CH-non-HDL, calculated GFR index, calculated BMI indicators, index of adaptive potential of the cardiovascular system CVS, and based on the obtained indicators and data analysis, risk factors and recommendations for their control are automatically determined, with the definition of targets for ideal weight, LDL levels, target blood pressure levels, uric acid, rehabilitation schemes and programs (physical activity, diet and calorie content with the calculation of the necessary basic metabolism, mental adaptation programs). This program and mobile application are convenient for working at the level of family clinics, as well as possible screening examinations of employees in organizations and educational institutions in order to early identify CVD risk factors. When creating the program, programs for working with the Website were used. Backed Laravel (PHP), Frontend React (Ant Desing), DB MYSQL, Android React Native (Webwiew). With the help of Backed Laravel (PHP), an interface user interface (MVC) platform for PHP, development was carried out in the PHP programming language and allowed the creation of a comprehensive program project and website. Laravel simplifies user practice by providing a wide range of features that automate programming and acceleration processes. Using Frontend React (Ant Desing), a JavaScript library, a programming platform that simplifies user creation and management. It is built into web application development thanks to its user-friendly and powerful component structure. React helps simplify development and distribution processes, improve usability, and improve integration with other web application components. Android React Native (Webwiew), a proprietary cross-platform environment for developing mobile applications based on JavaScript and the React library, is used, runs on iOS and Android platforms and is convenient for creating fast mobile applications. React Native makes it easy to create different mobile applications for both platforms by reusing JavaScript code and simplifies the development process by using React components.With the help of information technology and programming, the data obtained and recommendations for assessing CVD risk factors are systematized. Work has been carried out on the development of multifunctional platform-type services that combine not only data processing, taking into account modern recommendations for the prevention of CVD, but also the possibility of processing/transmitting information for further use. The program developed by us (mobile application) allows you to accumulate and track patient health data (CVD risk factors), store medical information, as well as analyze information with an assessment of goals and an assessment of deviations from clinical and laboratory parameters. Health status tracking: blood pressure, pulse, weight, stress level, indicators of clinical and laboratory parameters (glucose, cholesterol, LDL, CH-nonHDL, uric acid, calculated GFR index, calculated BMI indicators, index of adaptive potential of the CVS, CVR level indicator on the SCORE2 scale), conducting a rehabilitation program. The application implements a functional platform related to the diagnosis of heart diseases and the determination of stress levels, calories, determination of physical performance, activity tracking, psychological status, heart rate, monitoring of weight and body composition, respiratory disorders by peak exhalation rate, hypertension control, diet, calculation of BMI values, calorie intake. The "CVD Prevention School" included the following classes: Risk factors for cardiovascular diseases; Obesity, types of obesity; Arterial hypertension, dyslipidemia, disorders of carbohydrate metabolism; non-drug methods of prevention and treatment of CVD and metabolic syndrome: dietary approaches; non-drug methods of prevention and treatment of CVD: optimization of physical activity; psychological approach to CVD prevention. The initial clinical and laboratory parameters in both groups are presented in Table 1.
|
4. Conclusions
- Thus, a computer personalized individual health card and a mobile application developed on the basis of the card will optimize the work of doctors in polyclinics, and will also contribute to the introduction of innovative technologies in the primary health care sector.
5. The Results of the Study
- Based on the results of the study, diagnostic tables have been developed to determine the overall individual cardiovascular risk (CVR) and programs have been developed to determine the risk group: minimum, medium, high and very high risk, prognostic adverse signs have been identified, physical and psychological rehabilitation programs and principles of rational nutrition have been developed with the selection of individual schemes with the calculation of the required calorie content per day. A program has been developed for the mobile application of a personal health card and an individual wellness program.