-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(4): 1084-1089
doi:10.5923/j.ajmms.20241404.59
Received: Apr. 1, 2024; Accepted: Apr. 21, 2024; Published: Apr. 22, 2024

Conservative Treatment Tactics in Chronic Tendinopathy of Biceps Longus and Rotator Cuff Tendons
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIrismetov Murodjon Ergashovich1, Hamroyev Shaxzod Farhodovich2, Shamshimetov Dilshod Fayzaxmatovich3, Tadjinzarov Murodjon Baxodirovich2, Rustamov Firuz Faufovich2, Safarov Muxammad Mahmudovich2
1Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics of Uzbekistan, Director, Uzbekistan
2Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics of Uzbekistan, Traumatology and Orthopedics Doctor, Uzbekistan
3Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics of Uzbekistan, Head of Sport Trauma Department, Traumatology and Orthopedics Doctor, Uzbekistan
Correspondence to: Hamroyev Shaxzod Farhodovich, Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics of Uzbekistan, Traumatology and Orthopedics Doctor, Uzbekistan.
| Email: |  |
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective: Currently, the use of blood plasma saturated with platelets, that is, prp therapy, is becoming more and more relevant in the case of degenerative destructive changes in the knee joint and other large joints. PRP therapy in degenerative processes in the shoulder joint is now becoming a more relevant topic. Purpose: to study the effectiveness of prp therapy in patients with tendinopathy of the long tendon of the biceps muscle and rotator cuff muscles. Materials and methods of the research: the article is about the effectiveness of using prp in 112 patients who were treated as outpatients and inpatients in the Arthroscopy Department of the RSSPMCTO clinic during the year 2022-2023, 48 of the patients were male and 64 were female, and the average age was 51.8±7.6. Patients were divided into 2 groups: main (56) and control (56). The main group of patients received prp treatment in addition to the intra-articular NSAID that the control group received. Among them, 51.8% of patients had rotator cuff tendon tendinopathy, 25% had subacromial impingement syndrome, 32.2% had biceps tendon tendinopathy. The effectiveness of the treatment was evaluated on the basis of VASh, DAsh and UCLA scales before and after conservative treatment, as well as after 6 months. Results: in both groups of patients, after conservative treatment, it was found that pain decreased and range of motion increased. All main group patients had better results compared to the control group according to VASh, DASh, UCLA scales. During the post-treatment MRI and Ultrasound examination, it was found that the structure of the muscle tendon has improved and the swelling has decreased. Conclusion: PRP therapy is effective in chronic biceps longus tendon and rotator cuff tendinopathy of the shoulder. This was shown by the reduction of pain syndrome in the shoulder joint of the patients and an increase in the range of motion.
Keywords: Biceps, Long head, Tendinopathy, Prp, Rotator cuff
Cite this paper: Irismetov Murodjon Ergashovich, Hamroyev Shaxzod Farhodovich, Shamshimetov Dilshod Fayzaxmatovich, Tadjinzarov Murodjon Baxodirovich, Rustamov Firuz Faufovich, Safarov Muxammad Mahmudovich, Conservative Treatment Tactics in Chronic Tendinopathy of Biceps Longus and Rotator Cuff Tendons, American Journal of Medicine and Medical Sciences, Vol. 14 No. 4, 2024, pp. 1084-1089. doi: 10.5923/j.ajmms.20241404.59.
1. Introduction
- Pain in the shoulder joint is a common problem in the population, and according to various literature, it can be found in 17-47% of the population. This indicator increases with the age of the patient and is most common in patients aged 45-64. But only 1% of patients over the age of 45 turn to doctors for this pain [1,2].Pain in the shoulder area can be caused by various causes, among them, osteochondrosis of the cervical spine, shoulder-scapular joint, acromion-humeral joint, rotator cuff and other soft tissue pathologies in the shoulder area may be the cause. But among them, the most pathologies are related to changes in joints, accounting for almost 60% of shoulder pathologies [2,3,4].The term "tendinopathy" is a broad concept, and in recent years, the inflammatory nature of tendinopathy has been increasingly questioned. New theories show that only the etiological factors and pathophysiological mechanisms related to the inflammatory process cannot fully represent the complex processes in tendinopathies. Hypoxia, hyperthermia, apoptosis, effects of inflammatory mediators, and theories such as lactic acid ("oxidative stress") have not yet been fully proven [1,6].Tendinopathy of the shoulder joint occurs in 15-20% of people who engage in regular physical activities. One of the main causes of rotator cuff tendinopathy of the shoulder is subacromial impingement syndrome, which occurs in 18% of adult athletes whose main training activities involve loads involving the shoulder joint. Due to the high anatomical and functional correlation, tendinopathies of the shoulder biceps muscle occur in 41% of shoulder rotator cuff pathologies [4].In tendinopathies, there are some changes in the tendon. Of these, the tendons, which are normally white and shiny, turn gray-brown in tendinopathies. There are also changes in the form, diffuse or oval thickenings are found on the groin. In this case, histological examinations did not reveal any inflammation-related cells or signs in the tissue structure and composition. Disorientation, thickening, shrinking of collagen fibers against the background of blood vessel growth, increase in the number of cells, increase in the amount of glycosaminoglycans indicate the degenerative nature of the process. For this reason, the term tendinopathy is used synonymously with the term "tendinosis" in most literature [4,5,6,7,8,9].In tendinopathies, the absence of inflammatory symptoms and the absence of mechanical injury, but the appearance of a painful syndrome, is expressed by the increase of chemically active substances such as glutamate, lactate, substance R, neurotransmitters and their effect on nerve endings [10,12].Most often, tendinopathies pass without any clinical signs and can only become apparent when a partial or complete tendon rupture occurs. Such a condition is often found in pathologies of the rotator cuff in the shoulder joint. Pain appears to be the main symptom of paratendinopathy when the tendon is surrounded by paratenon, morphologically showing signs of inflammation. Biceps tendinopathy is a good example of this [10,11,12].Due to its positive effect on the inflammatory process, pain-relieving and reparative effect, PRP (platelet-rich plasma) therapy has shown good results in tendinopathies of various localizations, characterized by a predominance of the degenerative process and a slow recovery process [13,14,15,16].The results of conservative treatment of tendinopathies depend on various factors, among which the anatomical and biomechanical properties of the tendon, as well as the method of prp therapy, are of great importance. This factor is the basis for a good therapeutic effect in tendinopathies of the Achilles tendon, knee cap, and is the basis for some scientists to question the effectiveness of prp therapy in rotator cuff tendinopathies [6,14,17,18,19].Taking this into account, evaluating the effectiveness of prp therapy in various tendinopathies of the shoulder joint has not lost its relevance until now.The purpose of the study: to study the effectiveness of prp therapy in patients with tendinopathy of the long tendon of the biceps muscle and rotator cuff muscles.
2. Research Materials and Methods
- Materials on patients were obtained from 112 patients who were treated as outpatients and inpatients during 2022-2023 in the Department of Arthroscopy of the Republican Specialized Scientific And Practical Medical Center Of Traumatology And Orthopedics (RSSPMCTO) clinic. 48 of the patients were male and 64 were female, and the average age was 51.8±7.6. Patients were divided into 2 groups: main (56) and control (56). Among them, 51.8% of patients had rotator cuff tendon tendinopathy, 25% had subacromial impingement syndrome, 32.2% had biceps tendon tendinopathy.
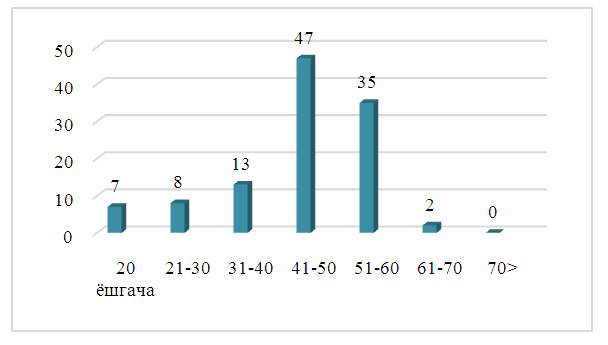 | Diagram 1. Distribution of patients by age |
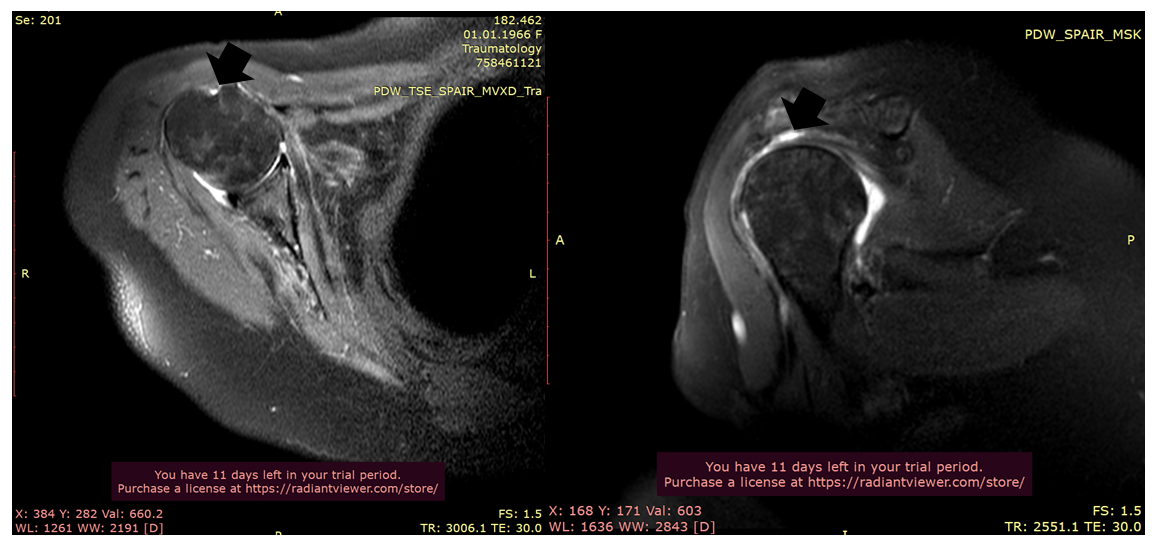
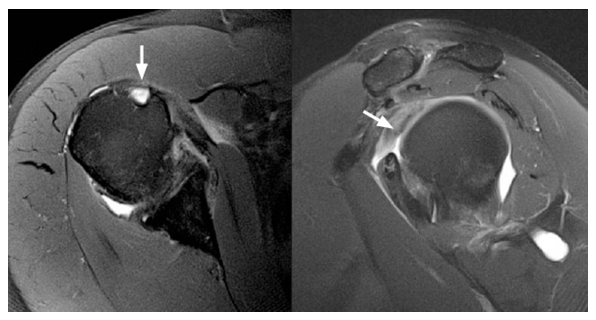 | Figure 1. MRI examination in tendinopathy of the biceps longus of the shoulder |
3. Research Results
- Before starting treatment, all patients had pain in the shoulder area lasting more than 3 months, intensification of pain when raising the arm above the shoulder level, and decreased range of motion. Neer injection test was positive in all patients. In this case, 10.0 ml of 1% Novacain solution was injected into the subacromial cavity.The average concentration of platelets in prp was 940±120×10³/μl. A high concentration of leukocytes was also detected in it - 22.4×109/l±7.8.When comparing the scores of patients in the main group and the control group on the above scales, patients who received prp therapy had better results in all indicators.
|
|
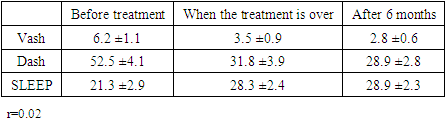
 | Figure 2. Patient A.K., 67 years old, MRI of biceps long head tendinopathy inspection |
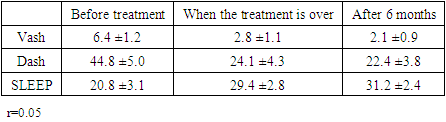
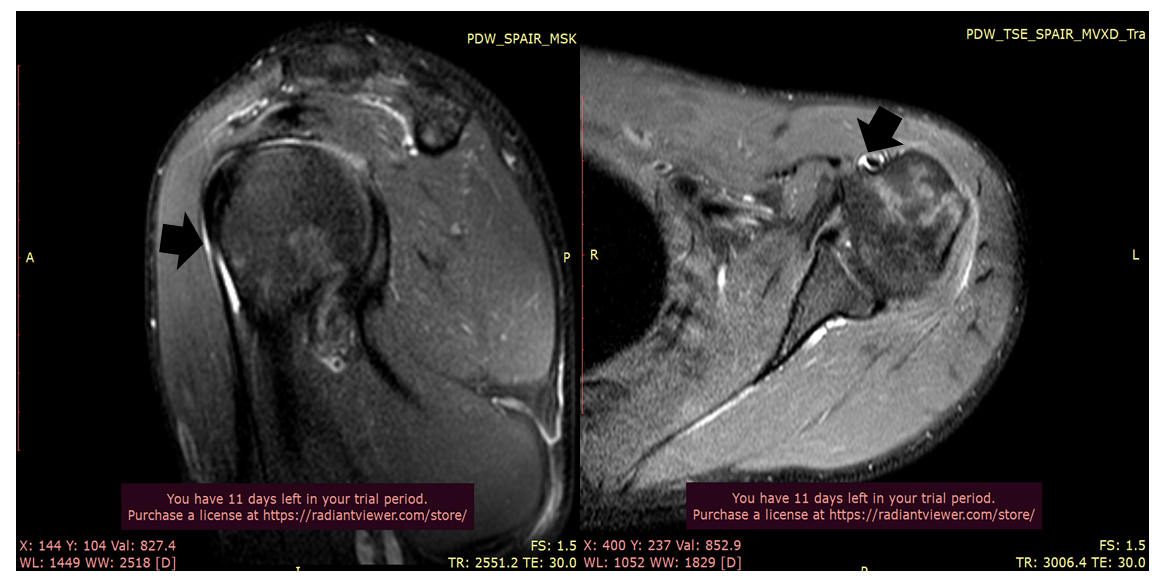 | Figure 3. Patient X.I., 35 years old, MRI examination of biceps longus tendinopathy |
4. Summary
- Treatment of tendinopathies of different localizations usually includes measures such as reduction of physical loads and limitation of movement in the joint of this segment, physiotherapeutic procedures, use of painkillers and anti-inflammatory drugs. Often, in the acute course of the disease, the clinical effectiveness of the above treatment procedures is high, but in the later course of the disease, with the degenerative nature of the treatments, its pathogenetic effect at the molecular, cellular level has not been clearly proven. Often, a small recovery of physical loads also causes the return of pain syndrome in the patient and the chronic course of tendinopathy [4,16,19].The specific properties of PRP allow the use of this blood product as a stimulator of the physiological and reparative processes of tendon tissue, not only conservatively, but also in tendinopathies treated by surgery [12,13,22,23].The results of several studies have shown that tissue growth factor in α-granules of prp has an effect on the transmembrane receptors of cells and the generation of intracellular signals, which regulates all 3 phases of the inflammatory process. The above factors in cells increase the synthesis of proteins that control the synthetic and proliferative functions of the cell through the expression of genes in the cell nucleus. In addition, the stimulation of the processes of chemotaxis, cell differentiation and local angiogenesis directly affects the healing process in the injured joint [7].As a result of the direct effect of PRP on tendon tissue, fibroblast proliferation, tenocyte and fibroblast synthesis of type 1 and 3 collagen, migration of stem cells from the bone marrow to the injured tendon, increase in the strength and size of the regenerate, improvement of the mechanical and histological properties of the bone-tendon junction are observed [13,14,15,22].One of the main indicators used in the classification of different types of prp is the concentration of platelets and leukocytes in the plasma. 4-5 times higher concentration of platelets, reaching 1000×103 μ/l, is considered a characteristic feature of prp [4,13]. However, until now, it has not been clearly proven that the high concentration of platelets in the plasma stimulates the reparative process. In addition, several randomized studies have shown that there is no clear correlation between the concentration of platelets in prp and the effectiveness of treatments [16]. This fact indicates a double effect of the growth factor on cell receptors: prp does not have a sufficiently stimulating effect at a low concentration, and on the contrary, an increase in the concentration of platelets above 1000×103 μ/l does not improve the regeneration process, but sometimes it is possible to slow it down [13]. In addition, the activity of some plasma proteins (IGF-1, HGF) does not depend on the amount of platelets. Thus, it was found that cell viability and proliferation decreased at high concentrations of prp, and increased at low concentrations [24].Opinions about the influence of the concentration of leukocytes in prp are relatively one-sided. A high amount of inflammatory mediators in plasma with a high concentration of leukocytes has a stimulating effect on reparative processes in chronic conditions such as tendinopathy [25,26]. Mononuclear cells have a positive effect on the activation of tissue growth factors due to the fact that they bind to the leukocyte fraction (lymphocytes and monocytes), most bioactive molecules, and even progenitor cells (CD34+) [27]. This suggests that a higher concentration of leukocytes in the plasma leads to a higher treatment efficiency. However, research shows that high isolation of the leukocyte fraction leads to a decrease in the concentration of platelets in the plasma. In our study, the average concentration of leukocytes was 24.7×109/l±8.6 [28].Another important aspect is the manipulation technique. Often, in tendinopathies, the injection is made directly into or around the affected tendon. But considering the thickness of biceps tendon structure, drug injections and prp were delivered to the subacromial space [18,28,29].Based on a prospective study conducted by M. Scarpone, injecting prp into the subacromial space, the patients examined pain, range of motion, and changes in joint structure on MRI. When the patients were re-examined after 52 weeks, they found that positive results were maintained in 94% of patients [3,12,26].DW Rha conducts a prospective randomized study in 39 patients. Patients are divided into 2 groups, and in patients, 2 times with a difference of 4 weeks, prp injection is sent to the tendon itself and around it. During the 6-month follow-up period, patients experienced an increase in pain and range of motion [18].Thus, prp therapy shows good results in the treatment of chronic tendinopathy of the biceps longus and rotator cuff tendons. These patients showed symptoms such as a decrease in pain syndrome and an increase in shoulder range of motion. The effectiveness of the treatment maintained its positive dynamics during the 6-month period.