-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(4): 944-950
doi:10.5923/j.ajmms.20241404.30
Received: Mar. 9, 2024; Accepted: Apr. 10, 2024; Published: Apr. 11, 2024

Improving Early Diagnosis and Prevention of Ischemic Heart Disease among Armed Forces Officers in the Republic of Uzbekistan
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMuyassar Gafurzhanovna Mukhamedova, Zikrulla Faizullaevich Niyazov
Military Medical Academy, Armed Forces of the Republic of Uzbekistan, and Central Military Clinical Hospital, Ministry of Defense, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Early diagnosis and prevention of cardiovascular diseases among officers in the Armed Forces of the Republic of Uzbekistan play a crucial role in enhancing troop combat readiness and mitigating disability resulting from ischemic heart diseases. Consequently, our research aims to identify officer patients who received outpatient treatment in the cardiology department of the Central Military Clinical Hospital and have a predisposition to ischemic heart disease. This allows us to form high-risk groups and implement primary prevention strategies for ischemic heart disease, emphasizing early diagnosis.
Keywords: Ischemic heart disease, High-risk groups, Risk factors, Primary prevention of ischemic heart disease, Lifestyle
Cite this paper: Muyassar Gafurzhanovna Mukhamedova, Zikrulla Faizullaevich Niyazov, Improving Early Diagnosis and Prevention of Ischemic Heart Disease among Armed Forces Officers in the Republic of Uzbekistan, American Journal of Medicine and Medical Sciences, Vol. 14 No. 4, 2024, pp. 944-950. doi: 10.5923/j.ajmms.20241404.30.
Article Outline
1. Introduction
- Cardiovascular diseases are a leading cause of premature mortality and disability in many countries, leading to a significant increase in healthcare expenditures. Atherosclerosis, which advances over several years before presenting specific symptoms, typically underlies the development of ischemic heart diseases. Sudden deaths resulting from myocardial infarction and stroke often occur without the possibility of providing prompt medical care, rendering most treatments ineffective or palliative. Modifying risk factors will undoubtedly yield reductions in mortality and morbidity [1,2,3,4].According to the 2018 report by the World Health Organization, over 17.8 million people worldwide die annually from cardiovascular diseases. Several objective factors contribute to the coinciding rise in the incidence and mortality rates of cardiovascular diseases: population aging, socio-economic factors, increased psychosocial stress, urbanization, dietary patterns, lifestyle changes, alterations in occupational activities, prevalent unhealthy habits, and unhealthy lifestyles among the majority of the population, including an unhealthy diet [5,6,7,8].The implementation of preventive programs has identified various factors that negatively impact their outcomes. These include a lack of awareness among the population regarding the possibilities of preventing cardiovascular diseases, passive participation or prolonged refusal to engage in preventive programs, especially among individuals who are seemingly healthy but possess risk factors, reluctance to modify lifestyles, and an increase in the morbidity and mortality rates of cardiovascular diseases, such as ischemic heart disease, following the discontinuation of long-term active preventive measures [9,10,11].
2. Research Objectives
- 1. Early diagnosis of ischemic heart disease among military personnel in the Armed Forces of the Republic of Uzbekistan.2. Prevention of ischemic heart diseases through the utilization of an electronic platform among military personnel in the Armed Forces of the Republic of Uzbekistan.
3. Research Goals and Study Subjects
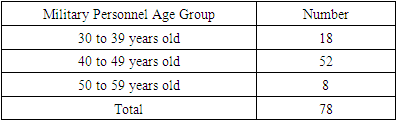
- The study subjects consist of 78 patients undergoing inpatient examination and treatment in the cardiology department of the Central Military Clinical Hospital. The brief description of the study includes patients' age, risk factors for ischemic heart disease, harmful habits, arterial blood pressure, measurement of total cholesterol (including low-density lipoproteins and triglycerides) in the blood, and primary and secondary prevention measures.The officers serving in the Armed Forces of the Republic of Uzbekistan are divided into three age groups:• Group I: 30-39 years old.• Group II: 40-49 years old.• Group III: 50-59 years old.Between April 2023 and December 2023, a total of 78 patients aged 30 to 59 years received treatment in the cardiology department of the Central Military Clinical Hospital.
|
4. Study Results
- Primary and secondary preventive measures aimed at mitigating the occurrence of ischemic heart disease were implemented among the selected group of 78 patients, as mentioned earlier. Atherosclerosis of the coronary vessels and elevated blood cholesterol levels are recognized as significant contributing factors in the development of ischemic heart disease. Hence, the primary objective of this study was to reduce the levels of blood cholesterol and its overall concentration. Additionally, modifiable risk factors among the patients included in the study were targeted for reduction and elimination. By addressing these factors, it is feasible to effectively prevent the onset of ischemic heart disease in this patient cohort.Group I consisted of officers between the ages of 30 and 39, totaling 18 individuals. Out of these patients, 16 were diagnosed with hypertension, 6 exhibited obesity levels categorized as I or II, 1 had type II diabetes, another was diagnosed with ischemic heart disease and painless myocardial ischemia, and 1 displayed an index score of 76 on the Agatston scale in the multispiral computed tomography (MSKT) screening. Furthermore, 3 individuals were diagnosed with other ailments. Among the smokers in this group, 3 exhibited atherosclerotic stenoses in the brachiocephalic vessels, while 2 presented similar findings within the masked group.Group II consisted of officers aged between 40 and 49, totaling 52 individuals. Out of these patients, 38 were diagnosed with hypertension and were constantly undergoing treatment for masked diseases. Additionally, 5 individuals were diagnosed with ischemic heart disease, and secondary prevention measures were implemented for these masked patients. One patient experienced an acute myocardial infarction, while another underwent coronary artery stenting. In addition, 4 patients were diagnosed with type II diabetes, and obesity levels categorized as I or II were detected in 17 patients. Among the masked group, 16 individuals were active smokers, and 6 patients displayed atherosclerotic stenoses in the brachiocephalic vessels, albeit at different percentages.Group III comprised officers aged between 50 and 59, totaling 8 individuals. Amongst these individuals, 7 were diagnosed with hypertension, 1 individual was diagnosed with type II diabetes, 1 person had ischemic heart disease, and 5 individuals displayed obesity levels categorized as I, II, or III. Atherosclerotic stenosis of the brachiocephalic vessels was detected in one patient, and one individual within the group was an active smoker. The findings indicate that the masked subgroup displays a significantly higher susceptibility to ischemic heart disease.To facilitate primary and secondary preventive measures for ischemic heart disease, these disease groups were consolidated onto a single electronic platform.For comprehensive risk assessment, it is recommended to employ the Systematic Coronary Risk Evaluation (SCORE). This new table, based on the findings of the SCORE study, offers numerous advantages. It was developed following a large-scale prospective European study and enables the prediction of atherosclerosis-related mortality risk over a ten-year period. The risk assessment comprises the examination of various risk factors, including gender, age, smoking habits, systolic arterial blood pressure, and the ratio of total cholesterol to high-density lipoprotein cholesterol. The evaluation of the overall risk of cardiovascular disease-related mortality for a decade is performed according to the SCORE system. Within the Maskur study, the total risk of cardiovascular disease-related mortality over a ten-year period is determined for officers.
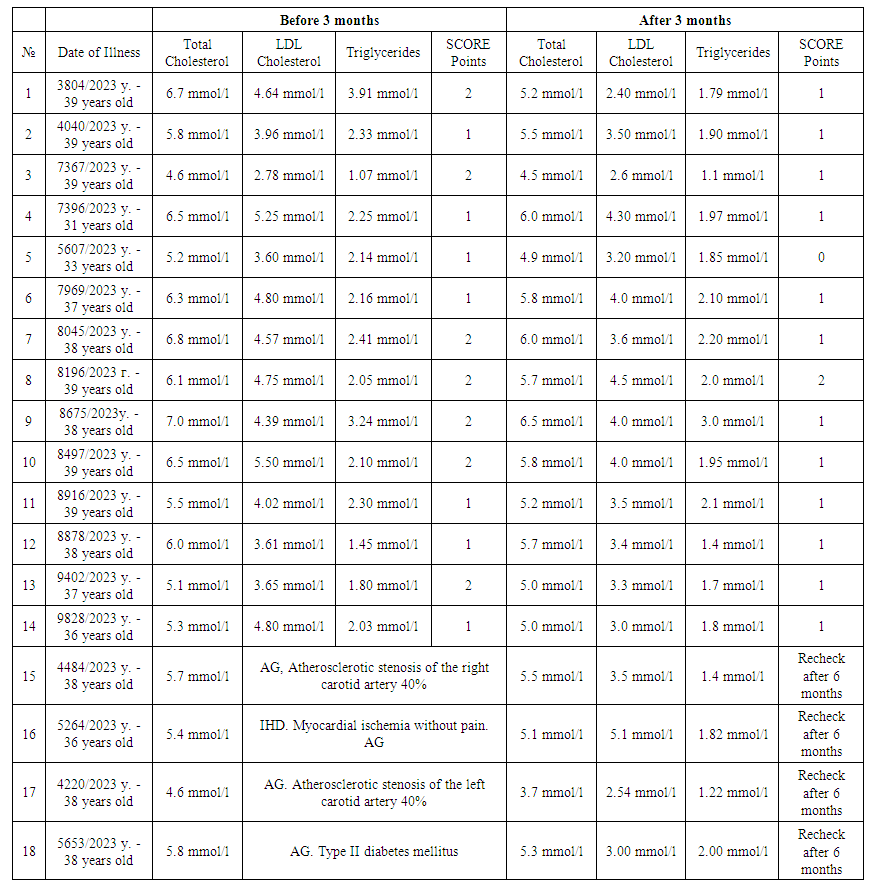 | Table 2. The results of the laboratory indicators of military personnel in 2023 |
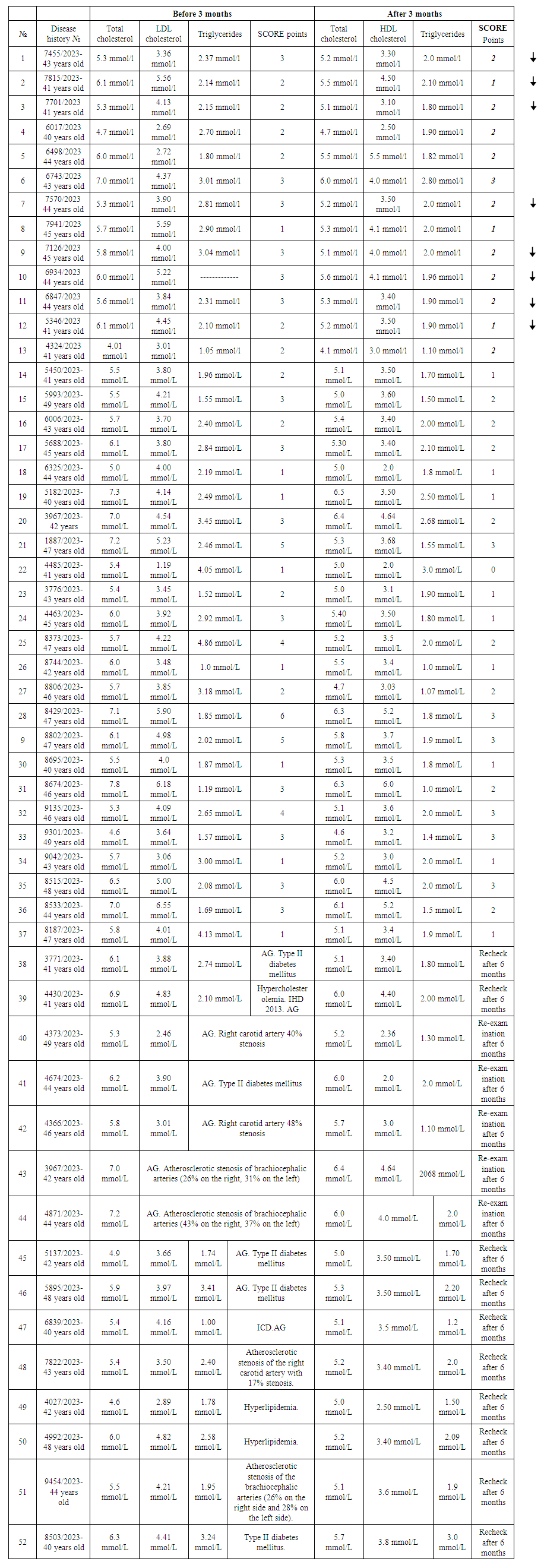 | Table 3. Assessment according to the scoring scale |
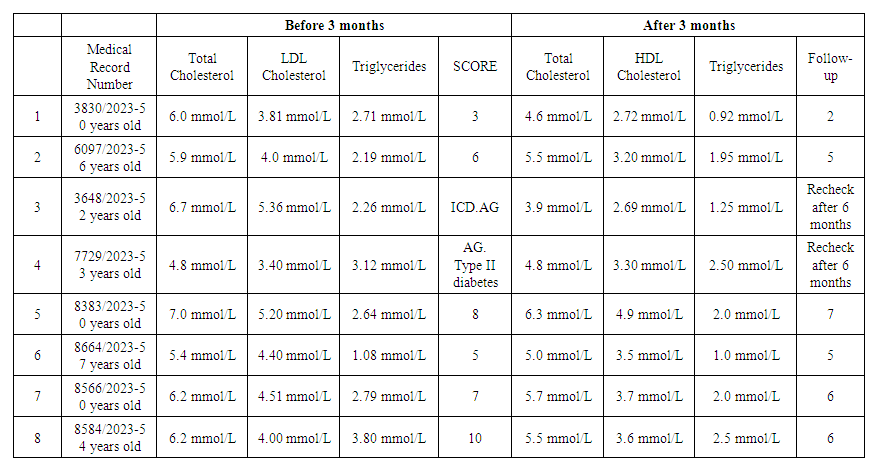 | Table 4. Assessment according to the scoring scale |