-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(4): 940-943
doi:10.5923/j.ajmms.20241404.29
Received: Mar. 12, 2024; Accepted: Apr. 8, 2024; Published: Apr. 11, 2024

Psychodiagnostics and Medical-Psychological Correction of the Screening of Children with Hyperactivity and Attention Deficit Syndrom
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMadirimova Latofat Ollaberganovna, Ibadullaev Bekzod Bakhramovich
Urgench Branch of Tashkent Medical Academy, Urgench, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

In this article, research has been conducted on the issues of conducting early screening and diagnosis of children with hyperactive and attention deficit syndrome based on new approaches, and providing effective medical and psychological assistance to children and their relatives.
Keywords: Hyperactivity, Lack of attention, Psychodiagnostics, Psychocorrection
Cite this paper: Madirimova Latofat Ollaberganovna, Ibadullaev Bekzod Bakhramovich, Psychodiagnostics and Medical-Psychological Correction of the Screening of Children with Hyperactivity and Attention Deficit Syndrom, American Journal of Medicine and Medical Sciences, Vol. 14 No. 4, 2024, pp. 940-943. doi: 10.5923/j.ajmms.20241404.29.
1. Introduction
- According to scientific sources and WHO data, various diseases and their syndromic manifestations are increasing among young children among the world's population today. Nowadays, one of the syndromes that has become one of the urgent medical-social and medical-psychological problems for children of kindergarten and school age and their relatives is hyperactivity and attention deficit syndrome (ADHD). Foreign and local epidemiological studies show that the prevalence of ADHD in our region ranges from 4 to 28%. The American Academy of Pediatrics (AAP) estimates that the prevalence of ADHD in children ranges from 4 to 12% [4]. [1,2,3,6]. Three groups of symptoms underlie the manifestation of attention deficit hyperactivity disorder (ADHD) in children namely: attention deficit, impulsivity and hyperactivity [4,5] At the same time, this syndrome is accompanied by a number of other medical and psychological disorders, i.e. oppositional disorders in 35% of children with ADHD, antisocial behavior in 26%, anxiety disorders in 26%, and depressive disorders in 18%, according to scientific sources [7]. The development of this syndrome in children, in turn, is considered one of the medical and psychological factors that cause a number of big problems for their parents and teachers. Therefore, early screening of hyperactive and attention-deficit syndrome (ADHD) in these children and correcting it in these children at an early stage is one of the urgent problems of today, and in turn requires scientific research [6,7].Purpose: Screening diagnosis of hyperactivity and attention deficit syndrome in children of kindergarten age and conducting medical- psychological correction in them.
2. Material and Methods
- During the years 2023-2024, 54 children who were brought up in preschool educational institutions and who were approached by their relatives with complaints related to hyperactivity and attention deficit syndrome were observed. The average age of the children was 4±1.5, of which 32 (59.3%) were boys, 24 (40.7%) were girls, and 25 children with no complaints related to the syndrome were included in the control group. 14 (56%) were boys, 11 (44%) were girls. The SADHD questionnaire specially adapted for parents was used by the authors in the screening diagnosis of hyperactivity and attention deficit syndrome in patients. Correction of psychoemotional and behavioral disorders developed in patients is carried out for two months on the basis of a medical-psychological algorithm consisting of two programs specially developed for children of kindergarten age, namely "program of fairy tales and stories" and "who is both an active and a passive program". The results were analyzed based on pre-treatment and post-treatment indicators using the SADHD-express questionnaire.
3. Results
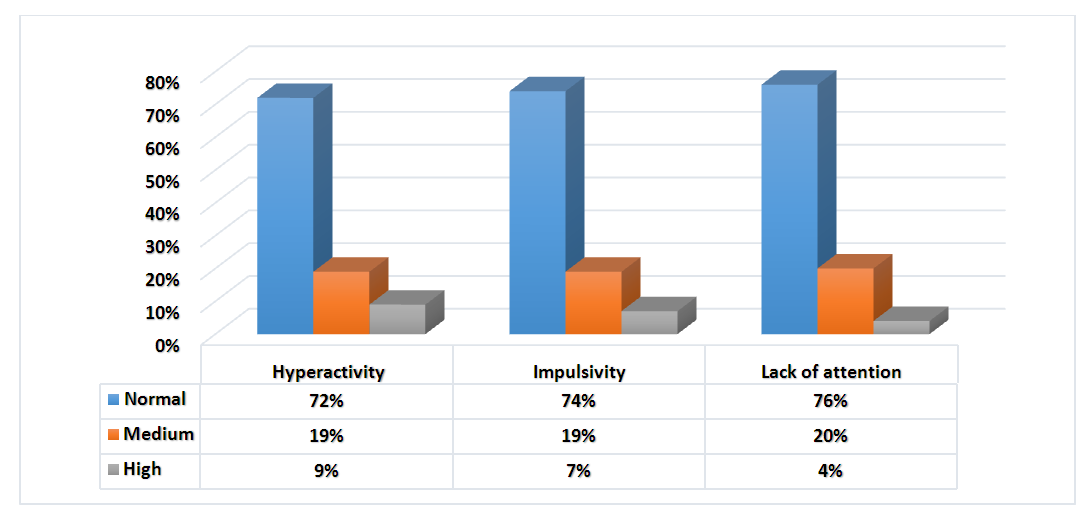
- The results of anamnestic subjective and objective complaints and psychodiagnostic analyzes before correction from the parents of the children in the 1st and 2nd groups of the observed children were as follows. According to it, the results obtained from our children's questionnaires were analyzed using the SADHD express questionnaire for the diagnosis of attention deficit hyperactivity disorder (ADHD) (Fig. 1).
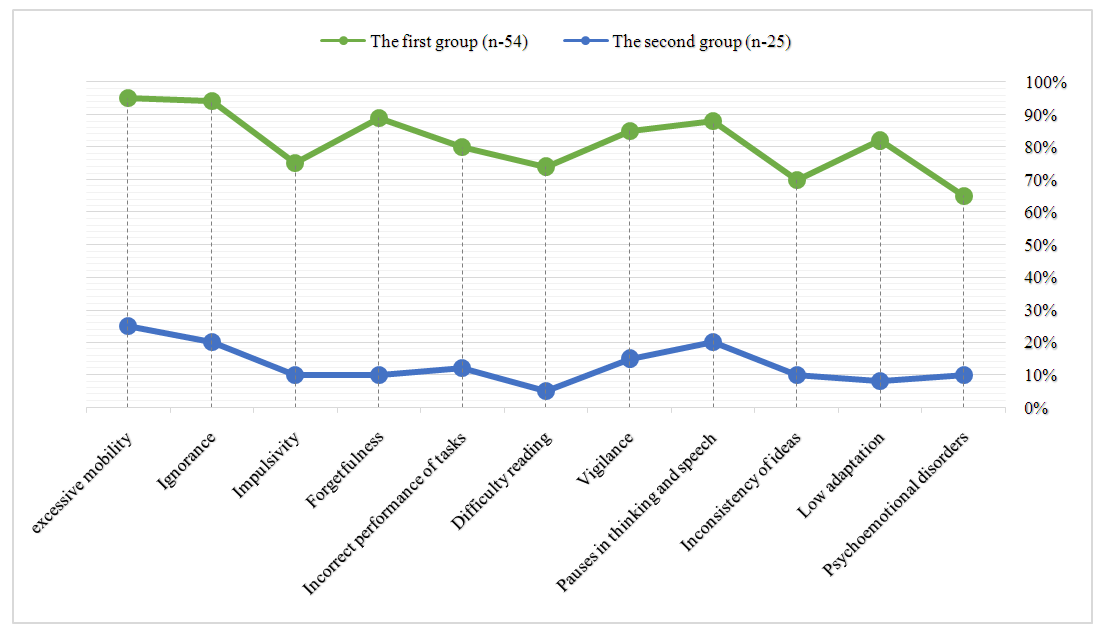 | Figure 1. Subjective anamnestic symptoms obtained from relatives of children in the main and control groups |
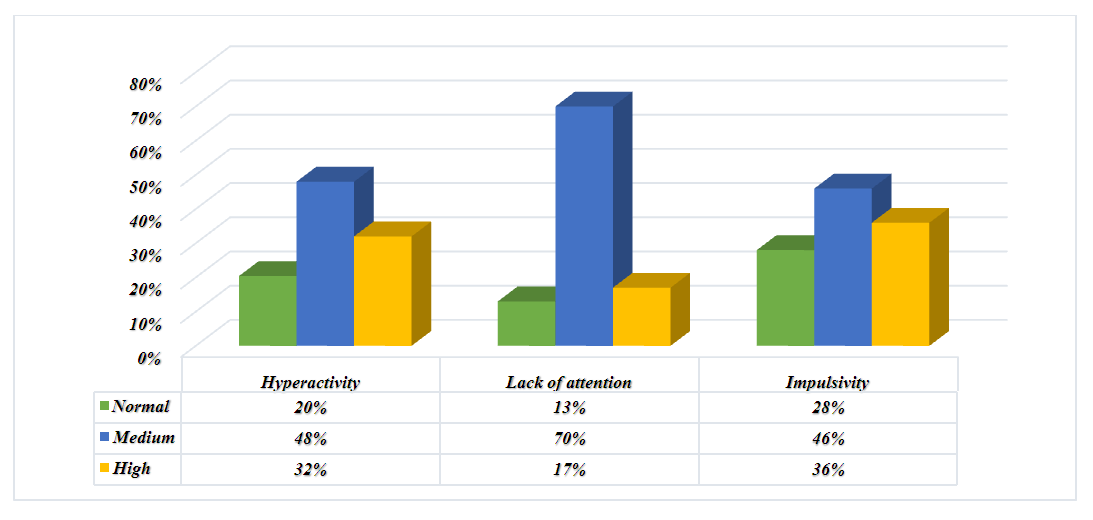 | Figure 2. Results of SADHD express questionnaire in children of the first main group before treatment (p>0.05) |
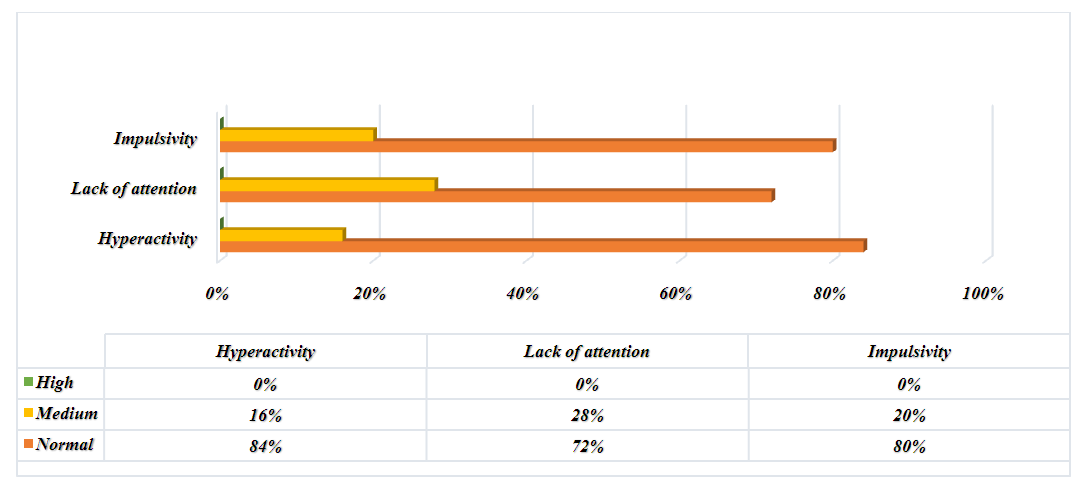 | Figure 3. Results of SADHD express questionnaire in children of the second main group before teatment (p<0.05) |
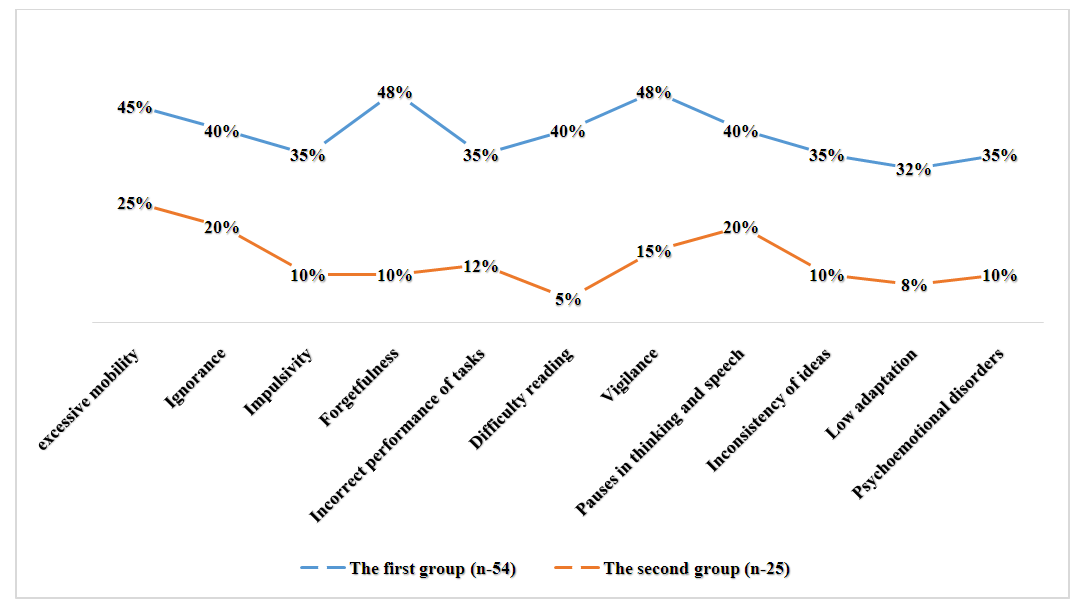 | Figure 4. Subjective anamnestic symptoms obtained from relatives of children in the main and control groups post- treatment |
 | Figure 5. Post-treatment results of the SADHD express questionnaire in children in the first primary group (p<0.05) |
4. Conclusions
- Based on the obtained results, it can be said that the SADHD-express questionnaire was the most effective method for the early psychodiagnostic screening of hyperactivity and attention deficit syndrome in children of kindergarten age, and the medical-psychological correction method consisting of special programs conducted in the second group of children and caregivers observed in our main group. we can see a decrease in complaints related to the syndrome. Thus, the psychodiagnostic and psychocorrective methods used in this work are used and implemented in children with developed hyperactivity and attention deficit disorder, it creates the ground for the mental and physical maturity of the growing generation, and the prevention of complications related to the syndrome.