Fozilov Uktam Abdurazzokovich
Associate Professor, Department of Orthopedic Dentistry and Orthodontics, Bukhara State Medical Institute, Uzbekistan
Correspondence to: Fozilov Uktam Abdurazzokovich, Associate Professor, Department of Orthopedic Dentistry and Orthodontics, Bukhara State Medical Institute, Uzbekistan.
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
One of the problems that must be solved is the occurrence of tooth-jaw anomalies in the pathology of children’s tooth-jaw system. From the first days of life, early orthodontic treatment for children with facial and jaw defects is a preparatory stage in the pre-operative period, aimed at creating favorable conditions for further surgical intervention. In early orthodontic treatment procedures, the jaw dimensions, the position of the jaws in relation to the base of the skull, the ratio of dental arches and the comparative diagnosis of tooth position defects are of great importance, and this article is about the solution of this issue.
Keywords:
Tooth-jaw anomalies, Deformation, Periodontium, Lip and palate
Cite this paper: Fozilov Uktam Abdurazzokovich, Comparative Diagnostic of Jaw Dimensions, Position of Jaws in Relation to the Base of the Skull, Proportion of Teeth Arches and Defects of Tooth Placement in Early Children, American Journal of Medicine and Medical Sciences, Vol. 14 No. 4, 2024, pp. 835-839. doi: 10.5923/j.ajmms.20241404.07.
1. Introduction
Until today, practical work on the treatment and prevention of dental diseases is being carried out. It is important to develop measures to prevent tooth-jaw anomalies from the embryonic period in carrying out complex measures aimed at the study and elimination of etiological and pathological factors. [1]. The incidence rate of tooth-jaw anomalies occurs in 50% of children, 30% of adolescents and adults [2]. The results of the researches conducted in the last ten years show that the downward trend in this indicator has not been fully determined [3].Teeth and jaws in children anomalies and deformations tooth diseases among caries and periodontal diseases after the third in place stands _ Their prevalence ranges from 11.4% to 80% [4].Congenital bilateral cleft lip and palate is the cause of teeth-jaw system anomalies in children in 12-25% of cases, and it is a severe type of tooth-jaw area pathologies [5]. Studying the frequency and distribution of dental-jaw system anomalies in children is one of the most important problems in modern dentistry [6]. One child in 1000 newborns is born with this anomaly, which is about 0.04% of the population of the planet [8]. Retention devices are used to prevent relapse and maintain results after orthodontic treatment of tooth - jaw system deformities in patients of different ages [7]. It is necessary to maintain the interocclusal height between the jaws, to control the vertical blocking of the incisors, that is, to act against the main pathogenetic mechanisms of the development of pathologies of the incisors [6]. The strategy of orthodontic treatment of tooth-jaw system deformations in patients of different ages and the choice of orthodontic devices depend on the etiological and pathogenetic components of certain tooth-jaw system pathologies. In addition, the correct selection of one or another orthodontic device depends on the condition of the oral cavity (GI) of the patient, the capabilities of the orthodontic laboratory and the professional skills of the orthodontist. In the period of persistent pricus, the common method of retention of the result of orthodontic treatment of the vertical occlusion of the incisors after treatment is the combined use of non-removable flex-retainers, which ensure the preservation of the new position of the teeth in the tooth rows, and bite plates to control the vertical occlusion of the incisors is one of the effective methods [9]. It is important to prevent pathologies of masticatory muscles that have a negative effect on patients with vertical occlusion of teeth.
2. The Purpose of the Study
Conducting a comparative diagnosis of jaw size, jaw position relative to the base of the skull, tooth arch ratio and tooth location defects in children with teeth-jaw anomalies or deformities.
3. Research Material and Method
The study included 440 orthodontic patients aged 4.5 to 18 years who applied to the Bukhara regional children's specialized dental center with anomalies and deformations of the tooth-jaw system. Orthodontic patient children were divided into groups based on age, sex, examination and treatment methods. Clinical examinations of 440 patients with pathological occlusion and teeth-jaw anomalies and deformations, etiological factors and childhood anamnesis were collected (from the first days), surgical operations in the face-jaw area during early childhood, infectious diseases and inflammatory processes were studied.
4. Research Results
It was important to study the condition of the patient's face and obtain its results in the comparative diagnosis of the jaw size, the position of the jaws in relation to the base of the skull, the ratio of the dental arches, and the defective position of the teeth in early-aged children. At this stage of the examination, the goal is to determine the characteristics of the patient's appearance based on defects. The face was viewed from the front and from the side. In the frontal view, the upper, middle and lower thirds of the face, their mutual proportions, nose-lip, lip-chin folds, chin protrusion were determined. The shape of the face is studied (wide, narrow, medium) and the Izar index is used. To do this, the length of the face was measured from the midline of the face to the gnatation point located under the chin along the midline. Then, the width of the face was measured from the point of bulge in the area of the cheekbones. The measurements obtained for the length of the face were divided by the width and multiplied by 100. Sizes of 104 and above reflected a narrow face, 97-103 corresponded to a medium face, and 96 and above corresponded to a wide face. The harmony of the medium face with macrodentia, and the narrow face matching the standard sizes of teeth (individual macrodentia) were identified as the reasons for the dense arrangement of teeth.Face check according to IzarDuring the external examination of the patient, the following was found:• symmetry of the left and right areas of the body and face;• correspondence of the midline of the face and body;Examination of the patient's face from the front shows:• face type from the front (narrow 104 and above, wide 97 and below, medium from 97 to 103);• facial symmetry;• According to Ilina - Markosyan, the shift of the chin to the left or right was studied;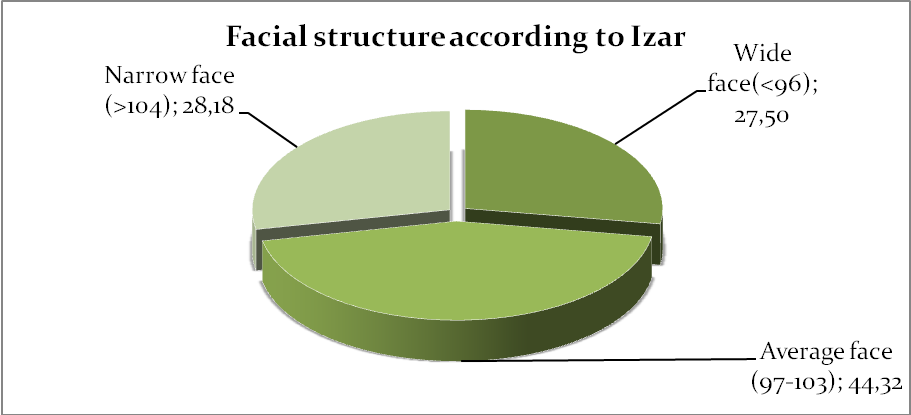 | Figure 1. Facial profile indicators according to Izar in the examined patients |
Changes in facial structure according to Izar in our examined patients were narrow face 28.18%, wide face 27.50%, average face 44.32%. Therefore, face profile verification was determined by the following methods.Examination of the patient's face in profile (from the side) shows the following:• type of face profile (straight, convex, concave);• position of the lips (protruding, retracting, normal);• state of the chin fold (lower jaw);During the oral examination, the following were studied:• dental examination (dental formula filled);• shape of teeth and alveolar walls was checked;• the location of the upper and lower lips, tongue tips was evaluated;• assessment of the location and size of the tongue (normo-, macro-, microglossia);• the configuration of the palate was studied.When assessing the condition of the temporomandibular joints (TMJ) of the examined patients, their functions were determined by the presence of occlusal defects, as well as the close relationship with the orthodontic treatment. The following cases were examined, which considered the main clinical symptoms characteristic of the pathologies of ChPJB.a) complete immobility – symptom of ankylosis;b) limitation of movement is a symptom of arthritis;c) increased range of motion is an exit symptom in arthrosis, typical for teenagersof pain when opening the mouth can be different. Arthrogenic pains associated with damage to joint elements (often the back parts of the joint bag) when opening the mouth are characteristic for joint pathology. Complaints of muscle pain based on tension and local spasms of masticatory muscles (external pterygoid, temporal, masticatory, internal pterygoid) were heard for painful dysfunction of the joint.Noisy conditions (rattling, rattling, loud crackling sound) were observed in various pathologies. Clinical analysis of the indicated symptoms has important differential-diagnostic value. Squealing and popping in the joint is a painful dysfunction of the joint, typical for teenagers and characteristic of arthrosis. The appearance of this symptom is explained by the increase in movement and "loosening" of the cervical spine, and the appearance of rattles is a change in the simultaneous movement of the disc and the joint head. According to most authors, the cause of rattles is the anterior displacement of the disc, as a result of which the joint head makes a sound when it passes along its rear thickened edge. When the mouth is closed, on the other hand, the articular head returns to its place first, and the articular disk remains late and enters the gap between the head and the condyle through the thickened rear edge during displacement, and it is learned to produce a characteristic sound.The patients under investigation were studied on the basis of simple and demonstrative samples using the Ilin a- Markosyan method.The first sample (study of the appearance in a calm state).The frontal and profile views of the patient at rest and during speech were studied: if the asymmetry was significant at rest and remained in the functional movements of the soft tissues of the face during speech, then strong changes in the development of one or both jaws were observed.Second sample (study of normal occlusion). The patient was advised to bring the teeth together in a comfortable position, including the lips (as he was used to): after that, the lateral displacement of the lower jaw was observed in some of our patients.The third sample (study of lateral movements of the lower jaws). Also, our patients were advised to open their mouths more slowly and their appearance was carefully studied: if the chin moved to the side while opening the mouth, the cause of asymmetry was the pathology of the temporomandibular joint.The fourth sample (relative study of normal and central occlusion). The patients were first asked to close their teeth in central occlusion, and then they were told to close it in a position that remained normal, and the appearance was compared from an aesthetic point of view: if the asymmetry was not noticeable in the position of the teeth closed in central occlusion, and it appeared only in normal occlusion, it was observed the causes of malocclusion. It should be said that in the case of masticatory muscle dysfunction and tooth row deformations, the patient did not always spread the tooth rows in the central occlusion.Assessment of soft tissues around the mouth. We used this method because 78% of our examined patients complained of changes in the soft tissues around the mouth. At this stage of the objective examination, the mucous membrane of the front of the mouth, its depth, and the condition of the lips are examined. The depth of the mouth was measured from the side of the lower lip with a special device. The depth is usually around 6-10 mm. We consider a pre-oral depth smaller than 5 mm to be small. Such a mouth was often observed in children with deep pricus. Examination of the oral cavity, condition of the mucous membrane, tongue, tonsils and larynx was evaluated. When the oral cavity was examined, the mucous membrane of the lung, the bottom of the oral cavity, the palate, and the tongue were thoroughly studied. The presence of tooth marks on the lateral surfaces of the tongue was found to increase macroglossia and its functions. This stage of the examination was completed by viewing the back wall of the larynx. Mucous membrane hyperemia, hypertrophy of lymphadenoid tissue and purulent secretions indicated the presence of an inflammatory process in the nasopharynx and larynx.Review of tooth rows. The examination begins with the examination of the teeth in the upper jaw, from right to left in the upper jaw, and then in the opposite order in the lower jaw. During the examination of tooth rows, attention was paid to the following cases:To determine whether each tooth belongs to a temporary pricus or a permanent pricus, to distinguish the structure of temporary and permanent teeth, the size, color, coating color, and the amount of bumps were taken into account.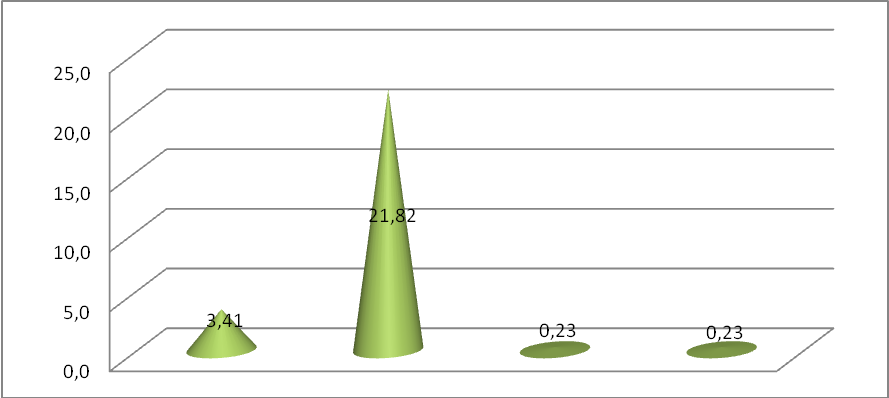 | Figure 2. Changes in the position of the chin based on the Ilina-Markosyan test in the examined patients. |
In our research, when examined by the Ilina-Markosyan test, 3.14% flattening of the chin, no change in 21.82%, 0.23% displacement, and 0.23% increase in displacement were found. In addition, assess the level of development of alveolar barriers in the front and side areas. In the occlusion of distal and deep scapular teeth, excessive development of the alveolar walls along the vertical line was observed from the front and underdevelopment in the lateral margin. It has been considered that incisor spade teeth have inverse proportions. Excessive development of the alveolar barrier is a sign of supraocclusion of teeth, and its underdevelopment is a sign of infraocclusion.Determining the shape and size of dental arches.Excessive development of alveolar walls in the sagittal direction usually leads to protrusion of teeth, while underdevelopment - retrusion of teeth and flattening of the dental arch were observed.The most responsible stage of the objective examination of the child consists of the following actions:- assessment of the relationship of the scapular teeth in the sagittal plane;- assessment of the ratio of shovel teeth in the transverse plane;- assessment of the ratio of shovel teeth in the vertical plane;- assessment of the ratio of the central lateral teeth in the sagittal plane;- assessment of the ratio of the central lateral scapular teeth in the transverse plane;- assessment of the ratio of the central lateral teeth in the vertical plane.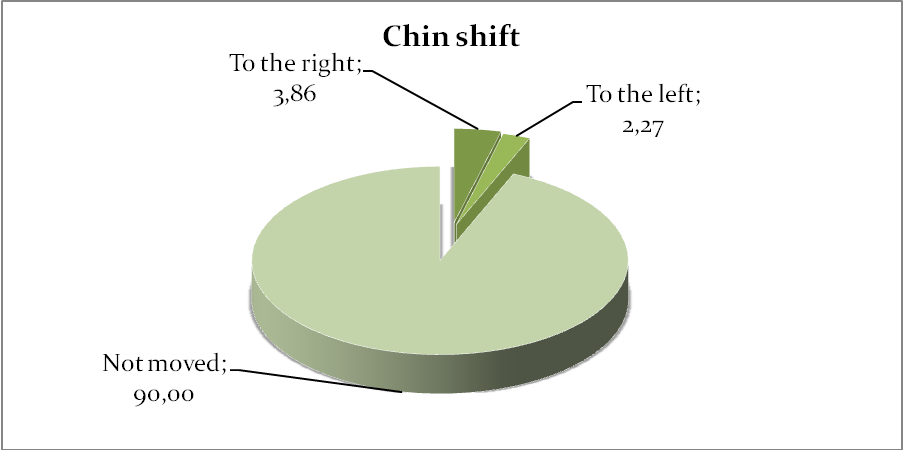 | Figure 3. Criteria for determining chin displacement |
In the examined patients, the criteria of chin shift in dentition defects was observed to be 3.86% to the right and 2.27% to the left. It was found that 90% of our patients did not move their chin.Assessment of the ratio of scapular teeth in the sagittal plane.As a rule, the upper incisors are located in front of the lower incisors, between them there is an incisor-cone relationship. The location of the lower shovel teeth ahead of the upper ones was considered a symptom of a violation of the sagittal plane. Another symptom of the sagittal disproportion of the scapular teeth is the presence of a sagittal crack, the size of which depends on the degree of sagittal disproportion in the relative position of the scapular teeth. One or the other symptoms were also observed in malposition of incisors or malposition and development of jaws. For this reason, the indicated symptoms can be used only in the presence of other clinical symptoms, from the point of view of comparative diagnosis. The inverse ratio of the scapular tooth in alignment with the sagittal cleft was defined as the results of lower scapular tooth protrusion, upper scapular tooth retrusion, mandibular overgrowth, or mesial position.Evaluation of the ratio of shovel teeth in the transverse plane.In dental-jaw defects, the proportions of the middle lines are disturbed for various reasons, including the absence of one incisor tooth, incisor teeth location defects, retention of some frontal teeth, the presence of a tooth in an extremely dense set, displacement of the lower jaw was observed in our patients.Evaluation of the ratio of the central lateral teeth in the sagittal plane. This stage of diagnosis was considered decisive for determining the type of bite. The ratio of the central lateral incisors in the sagittal plane was evaluated based on the Engle classification - the ratio of the first permanent molars was evaluated.In the third group of patients with anomalies and deformations of the tooth-jaw system, 28% of our patients had the presence of the second class according to Engl, a diagnostic sign of distal occlusion, and the clinical form of the defect was determined. It was conducted on the basis of teleroentgenogram analysis of the issue.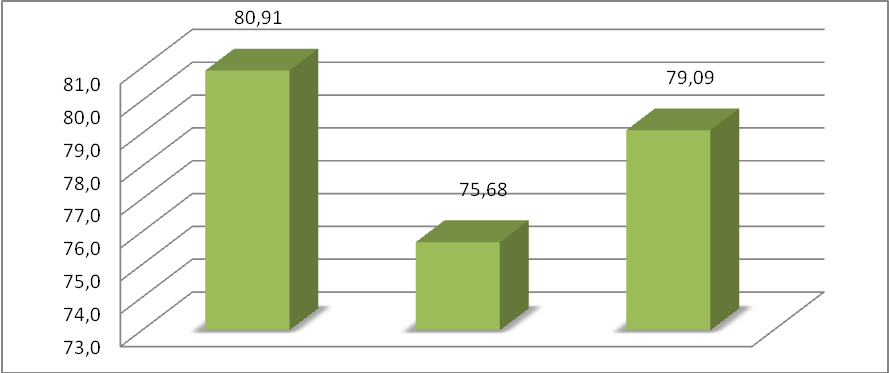 | Figure 4. Tooth-jaw anomalies and deformities, jaw conditions, tooth row defects |
Among the examined patients, changes in teeth row defects were observed in 80.91% cases of symmetrical face, 75.68% deepening of the chin cavity, and 79.09% cases of lip closure.If the mesial-protruding round of the first upper molar is located distal to the first transverse ridge of the antagonist-tooth, the third class according to Engl is recorded as the main diagnostic symptom in the mesial occlusion of tooth rows. However, here the ratio of the front teeth can be broken in one, two or three planes. It is difficult to establish the clinical form of mesial occlusion without teleroentgenogram analysis. In some cases, the following clinical method helps: the patient is advised to open his mouth a little, and then slowly close the mouth, raising the tip of the tongue to the palate (in this case, the patient can put some pressure on the chin). If he can set the spade teeth according to the principle of correct occlusion, then the mandible is assumed to be prognathic, that is, the anterior position of the mandible (the "joint" form of mesial occlusion). This model is not used in other clinical forms of this disease.It should be taken into account that the ratio of the first permanent molars on the right and left sides may be different. For example, the right side may belong to the first class, while the left side may belong to the second class. Such situations occur more often in the reduction of the tooth row, adentity and retention of premolars, "hiding" of the original class with another. For this reason, in each case, it is necessary to carefully analyze the jaw models and avoid errors in their identification.
5. Conclusions
The advantage of these methods is that the patient's mental state is not negatively affected during the examination. At the same time, it allows to correctly and effectively determine the etiological factors that have an adverse effect on permanent teeth pricus. Based on the results of the research, the best way to correct the pathology of the bite is during the period of tooth replacement, which often excludes the need for treatment in older children. The results of early treatment are more stable and rarely recur, as it has been found to be related to factors such as the development of growing tissues, tooth eruption, and the growth of alveolar barriers in root formation.
References
| [1] | Axmedjanovna, Yunusova Umida. "Diagnosis and combined treatment of temporomandibular joint." Eurasian Scientific Herald 15 (2022): 5-10. |
| [2] | Zubareva A. V., Garaeva K. L., Isaeva A. I. Rasprostranennost zubochelyustnyx anomaliy u detey i podrostkov (obzor literatury) // European research. – 2015. – no. 10 (11). - S. 128-132. |
| [3] | Sharipovich, O. S., Baxtiyorovich, B. B., &Ahmadjonovna, Y. U. (2021). Features of the course of the carious process in children with dentoalveolar anomalies in the bukhara region. Journal of Natural Remedies, 21(12 (2)), 27-33. |
| [4] | Fozilov, U. A. "Diagnostics and prevention of the development of caries and its complications in children at orthodontic treatment." JournalNX 6.07 (2020): 276-280. |
| [5] | Olimov, S. Sh, J. N. Bakaev, and U. A. Yunusova. "Factors of Non-Specific Protection of Oral Fluid in High School Children with Dental Anomalies." Middle European Scientific Bulletin 16 (2021). Stepanov K. E., Fadeev R. A. The effect of orthodontic treatment on training activity and functional parameters of external breathing and sportsmen with dental anomalies //Institut stomatologii. - 2019. - No. 1. – S. 64-67. |
| [6] | Khabilov N. L., Nurova Sh. N., Nurov N. B. Prevalence of dental anomaly in children of school age in Bukhara region // Mejdunarodnyi journal prikladnyx i fundamentalnyx issledovaniy. – 2015. – no. 12-9. - S. 1633-1634. |
| [7] | Durdiev J.I., Gaffarov S.A., Olimov S.Sh. Morphometric features of the dentition in children with chronic diseases of the upper and middle respiratory organs // Uzbek Medical Journal. – 2020. – №3. – C. 28-32 (14.00.00; №8). |
| [8] | Fozilov U. A. Prevention of caries development during orthodontic treatment // World Bulletin of Social Sciences. – 2021. – Т. 3. – №. 10. – С. 61-66. |
| [9] | Fozilov U. A., Sh O. S. Improving The Treatment of Abnormal Bite Caused by Severe Damage To The Jaw // Journal of Advanced Zoology. – 2023. – Т. 44. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML