-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(4): 808-812
doi:10.5923/j.ajmms.20241404.02
Received: Feb. 23, 2024; Accepted: Mar. 22, 2024; Published: Apr. 1, 2024

The Modern Problems of Anthropometric Indicators of Schoolchildren
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLTuymachev A. Ulmas, Tastanova E. Gulchehra, Khatamov I. Alijon, Ubaydullaev L. Rustam, Zafarova Z. Nusratoy
Kimyo International University in Tashkent, Tashkent State Dental Institute, Tashkent Pediatric Medical Institute, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The paper presents data from anthropometric studies of school-age children in rural areas of the Tashkent Region. The indicators of age-related dynamics were studied and the periods of the greatest increase in the morphometric indicators of school-age children were determined.
Keywords: Anthropometric indicators, Morphometry, Schoolchildren
Cite this paper: Tuymachev A. Ulmas, Tastanova E. Gulchehra, Khatamov I. Alijon, Ubaydullaev L. Rustam, Zafarova Z. Nusratoy, The Modern Problems of Anthropometric Indicators of Schoolchildren, American Journal of Medicine and Medical Sciences, Vol. 14 No. 4, 2024, pp. 808-812. doi: 10.5923/j.ajmms.20241404.02.
Article Outline
1. Introduction
- Regional norms and standards using the anthropometric method worldwide, including in Uzbekistan, several scientists have carried out scientific research on the identification and evaluation of the morphometric characteristics of children's physical development for development however, scientific data on the morphometric parameters of the body parts of children living in rural areas are rare, and studies aimed at studying their relationship with lifestyle and conditions have not been conducted. Thus, it is necessary to study the changes in the morphometric indicators of body parts of schoolchildren living in rural areas depending on age, to develop normative national standards for morphometric parameters, and to continue studying the relationship between morphometric indicators of school-aged children and their physical development patterns.
2. Aim of the Research
- Analysis of anthropometric indicators of schoolchildren living in rural areas.
3. Methods
- An analysis of the dynamics of anthropometric indicators of more than 1050 school-age children in the Tashkent Region aged 7 to 16 years was carried out. Each age group of students included more than 100 boys and girls. The method of parametric statistics was used to calculate such indicators as the arithmetic mean (M), its error (m), and standard deviation (δ). Indicator M±δ is the area of average values characteristic of the parameters of normal values. In this case, M+1δ is the upper limit of the norm, M-1δ corresponds to the lower limit of the norm. In our study, non-parametric evaluation criteria were also used – centile tables. The entire variation series was divided into 8 centile scales. 4-5 intervals are taken as the norm. Indicators falling into the 4-5 intervals are assessed as average. The values of interval 3 are interpreted as reduced, interval 2 – low, interval 1 – very low. The 6th interval indicates increased, the 7th interval – high and the 8th interval – a very high value of the indicator. The performed centile distributions of anthropometric data indicators most objectively reflect certain characteristics and their deviations at different ages. At the same time, centile distributions can be used to determine the somatic body type. The harmony of children's development can also be assessed using centile scales. The somatotype was determined by the sum of the numbers of “regions” or corridors of the centile scale. With a score of up to 10, a microsomatic body type was considered. From 10 to 15 points – a group of metasomatic physique, and from 16 to 21 points – a group of macrosomatic physique. In all the study groups, the 3 centile indicators “weight, standing height, chest circumference” were summed up. When determining the harmonious development, the centile indicators of weight, standing height, and chest circumference were also compared. Moreover, if in each case three indicators were included in the same centile or the difference between them was 1, the development was considered harmonious. If the difference between the three indicators is 2, it is moderately disharmonious. If the centile groups according to the compared indicators were included in different groups and the difference in centiles exceeded 3, severe disharmony was diagnosed. A detailed analysis of the variation series corresponding to each age and sex range was carried out. For this purpose, the values of anthropometric indicators related to each age group were divided into separate groups: group 1 included indicators located below the low limits of the norm-values below M-1δ; Group 2 included values within the normal range-indicators corresponding to M±1δ; Group 3 included values exceeding the normal range-more than M+1δ.
4. Results
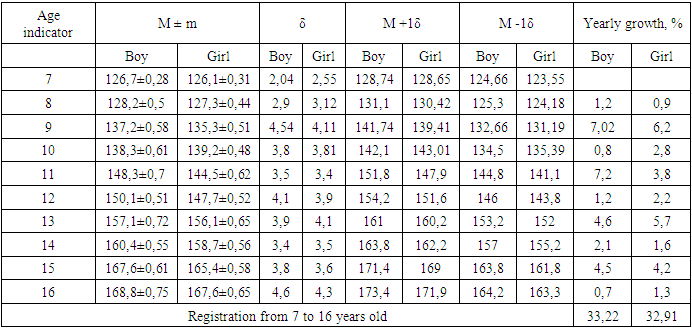
- Analysis of statistical parameters showed that the weight of the examined children undergoes ambiguous changes with increasing age. Boys and girls at the age of 7 were characterized by relatively similar body weight. Up to the age of 16, the body weight of boys increased by 129,7%; in girls, the weight gain corresponded to 128,2%. Annual weight gain in boys and girls is uneven. For boys between 7 and 8 years of age, the increase was 13,9%, and for girls – 8,6%. The most effective increase in body weight in boys was found in the period between 10 and 11 years – 20,7%. In girls, the greatest annual weight gain was detected between the 10th and 1st years of age – 15,6 %. In girls, there was also a second increase in annual weight between the 13th and 14th years – 12,4%, while in boys the annual increase starting from the age of 12 was relatively stable. Analysis of the data obtained showed that in all groups of examined children there is a tendency towards growth dynamics. Boys included in group 1 (the group with lower values of the normal corridor), up to the age of 16, body weight increased by 154,05%. The 2nd group of boys (normal range) increased by 159,7% by the age of 16. The group of boys exceeding the norm by the age of 16 gained 119,6%. Analysis of the dynamics of changes in the weight of girls by group also indicates that the group with less weight and those with weight within the norm corridor gained more weight by the age of 16. The weight of girls whose weight was below the normal range increased by 147,2% by the age of 16 compared to the indicators at 7 years of age. The second group of girls (corridors of the norm) weight increased by 138,65% by the age of 16. The third group of girls (whose weight exceeded the normal range) by the age of 16 increased their weight by only 120,75%. The largest annual increase in all groups is for boys between 10 and 11 years, while for girls it is between 13 and 14 years. The number of cases within the normal range among girls occurred from 65,4% to 76%. In the group of girls examined, from 10% to 18,3% of cases with weight below the normal range were identified. The number of overweight girls (group 3) was detected from 11% to 19,5% of cases. The number of children exceeding the norm is from 11% to 19,3 cases. Comparing the indicators of age and sex groups, it can be noted that the number of boys outside the norm ranged generally from 24% to 37,2%, and in the girls group – from 24% to 34,6%.The statistics on the dynamics of height change of standing are presented in Table № 1
|
|
5. Discussions
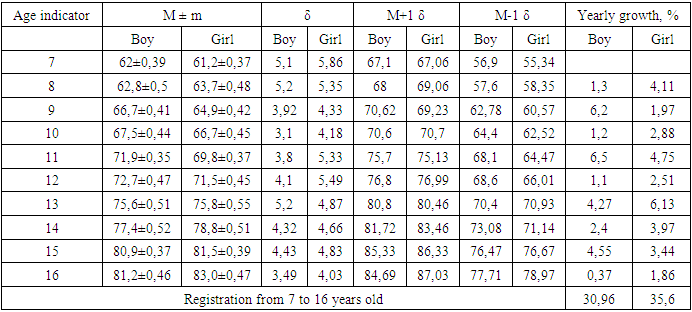
- Many researchers emphasize that the study of somatometric postnatal ontogenetic anthropometric parameters of the body leads to age-dependent, individual changes not only quantitatively, but also qualitatively. The comparative analysis of the studied age-related differences in the average body size of children of different groups of somatic development made it possible to identify not only gender differences but also the variability of growth processes in individual somatotypes. The trend that has emerged in recent years shows that low growth indicators are increasingly being detected in children of early puberty, which can be considered as one of the first signs of the slowing down of the growth process and the end of the acceleration processes. A disharmonic development trend was revealed. A large number of children who are overweight or underweight have been identified. Extreme variants of physical development began to be identified more often, and harmony indicators decreased. Taking into account the great informative value of physical development indicators, for the first time in European Union countries, data were published that simultaneously considered the life expectancy of adolescents and the increase in body length as equivalent generalizing parameters of health. According to the authors, one of the reasons for the decline in physical development is the decrease in the average number of children in the family. Body length and weight, as well as their proportions, are the most important integral signs of the morph functional state of a person throughout his life. For a newborn baby, body length and weight are the only criteria for the level of somatic maturity. To assess the physical condition of children, length, and body weight indicators are the basis for screening and are the most popular method of monitoring children's physical condition in modern pediatric practice. Deviations in the level of body length and weight values determined with its help (deficiency or excess) are often the first signs of functional disorders of the child's body or some diseases. The main dominant feature of the dynamics is the relative stability of the individual somatic condition in the general dimensions, length, and weight of the body, in boys and girls between the ages of 7-16. The disorder is partly due to the restructuring of growth in adulthood, partly due to the accumulation of random environmental influences. Changes in body length and weight occur during adolescence, especially in boys. Boys and girls aged 7-16 years have a constantly increasing level of body weight about its length, that is, a steadily increasing mass-height ratio. Currently, in economically developed countries, obesity is found in almost half of the adult population and 12-14% of the children. In schoolchildren, the mass of adipose tissue decreases with age, and in boys, there is an inverse relationship between this. The index of puberty, and for girls, the value of the relative mass of adipose tissue remains almost unchanged from puberty. Analysis of our data showed that the body weight of the examined children increased naturally with age. Thus, the increase in body weight in boys from 7 to 16 years old is 33,6 kg (129,7%), and in girls 32,7 kg (128,2%). Annual weight gain in boys and girls is characterized by uneven and different values. The most effective weight gain in boys was found at 11 years (20,7%), and in girls at 11 (15,6%). In girls, the second time weight gain was observed at the age of 14 years (12,4%), and in boys, the second time weight gain was observed at the age of 15 years (18,3%). The annual intersection of boys and girls is observed at the age of 10 and 14. This is Ashurov T.A. and others, where at 8 and 9 years old boys have more body weight than girls, and at 13 years old girls are 4,6 kg heavier than boys; At the age of 15, the second intersection of the growth curve is observed, and already at the age of 16, boys weigh 3,0 kg more than girls. According to our data, body weight increases by 17,1 kg in boys at 7-12 years, 17 kg in girls, and by 13,2 and 13 kg at 13-16 years, respectively. According to the literature, the average body weight of boys aged 16-21 years is significantly higher than that of girls by 21,4%. We agree with the opinion of several authors that the increase in body weight with age is necessarily related to the growth of muscle tissue and bone mass.The standing height of boys and girls increased by 33,22% and 32,91%, respectively, during the study period. The most effective growth of boys was recorded at the age of 9 (7,02%) and 11 (7,2%), and the age of 9 (6,2%) and 13 (5,7%) for girls. According to our data, the body size of boys and girls at the ages of 7 and 10 is almost the same. At all other ages (ages 11, 12, 13, 14, 15, 16), boys' body length is greater than that of girls. Our data differ from studies conducted in the cities of Minsk and Chelyabinsk, as well as in the Belgorod region, where the growth of girls aged 13 to 16 years is 9 – 13 cm. In our studies, the growth in boys from 7 to 12 years old is 23,4 cm, and in girls 21.6 cm, and from 13 to 16 years old it is 11,7 cm and 11,5 cm, respectively. In the studies of some authors, the intersection of the growth curves of boys and girls was observed at the age of 14, while in our research, the intersection of the curves was noted at the age of 10. According to, the fastest increase in the average growth rate of urban girls, was observed from 9 to 13 years old, and for rural girls from 9 to 12 years old. According to T.A. Ashurov, the standing height of 16-year-old boys is the same as that of girls. According to our data, the standing height of girls lags behind boys by 1,2 cm. This indicates that more accelerated shifts have been detected in rural children in the last decade. Intensive growth in boys is observed in our data at 9, 11, 13, and 15 years of age, and in girls, it coincides almost simultaneously and is observed at 9, 10, 11, and 13 years.In children of both sexes, the growth of all chest parameters (1,2 and 1,3 times) is observed at the age of 13-16. Thus, at the age of 7, the chest circumference indicators of boys and girls had the same parameters. From the age of 10, the parameters of the chest circumference of boys began to slightly exceed those of girls of the same age. The annual growth parameters were mostly dynamic in nature. The largest increase in girls was 4,75% at age 11 and 5,48% at age 13, while boys had 5,3% at age 9, 6,4% at age 11, and 7,8% at age 15. The overall increase in chest circumference was 30,9% for boys aged 7 to 16 years, and 35,6% for girls. At the age of 15-16, the chest circumference of boys exceeds that of girls. According to a number of authors, by the end of 12 years, the chest circumference increases by 7,0 cm in boys and 11,0 cm in girls. The increase in chest circumference between 8 and 13 years in girls and 10 and 15 years in boys is consistent with our data. Thus, according to our research, at the age of 7-12, the growth of the chest circumference in boys is 10,5 cm, and in girls it is 10,3 cm. From 13 to 16 years, the growth of the chest circumference is 5,5 cm in boys and 5 in girls. It was 7 cm. According to J.S. Soorbekov, at the age of 7-12 years, the circumference of the chest at the nipple level increases by 2,0 times in boys and 2,1 times in girls, which is significantly higher than our indicators. (according to our data, 1,19 and 1,17 times, respectively). In our opinion, this may be due to the fact that Kyrgyz children live in the middle mountains.Since the centile method is not limited by the nature of the distribution, it is suitable for evaluating any indicators. We also compared weight, standing height, and chest circumference to determine developmental consistency. Dorokhov R.N. proposed the definition of somatotypes based on the magnitude of sigma deviations of length, body weight, and chest circumference from the average values. According to the sum of the deviations expressed in points, the subjects are divided into three main somatic types – microsomal, mesosomal, macrosomal, and two transitional periods: micromesosomal and mesomacrosomal. The results of the statistical data of the somatotypes obtained by us, as well as the developmental harmony determined by the comparison of weight, standing height, and chest circumference are presented in the appendix. At the same time, the exact dynamics of changes in indicators depending on age have not been determined. Between 7 and 16 years of age, mesosomal body types were found in 59% to 75% of boys and 59% to 71% of girls. This corresponds to the data from T.A. Ashurov, in which 73,6% of children are characterized by a good level of physical development. Average disharmony rates range from 14% to 24% for boys and 17% to 30% for girls. We believe that it is necessary to pay attention to the obvious disharmony of situations among school-aged children. Disharmony was found in 6% to 15% of boys and 7% to 16% of girls. According to several authors, children with disharmonic development make up about 23,0%.
6. Conclusions
- 1. Total morphometric indicators and their segments increase intensively in schoolchildren living in rural areas compared to the age of 7 years. In particular, height increases by 33,2% in boys, by 32,9% in girls, weight by 129,7% in boys, and by 128,2% in girls. The most intensive growth corresponds to the contribution of long tubular bones.2. Acceleration of growth processes in boys is observed at 9, 11, and 15 years, in girls at 9, 13 years, and slowing down at 10, 16, and 12, 16 years, respectively: gender differences exist in 12-14-year-old children, and are determined in all anthropometric parameters of body parts.3. The distribution of physical development in students of different ages is as follows: harmonious development in boys from 59% to 76%, in girls from 58% to 72%; average disharmony is 15% to 25% in boys and 18% to 31% in girls; positive disharmony in 7% to 16% of boys and 8% to 18% of girls;4. The distribution of students of different ages by somatotype is as follows: mesosomal body type in boys from 60% to 77%, in girls from 58% to 72%, microsomal type in boys from 9% to 17%, and in girls from 7% to 14%, macrosomal the type is detected in 17% to 33% of boys and 19% to 31% of girls.