-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(3): 739-742
doi:10.5923/j.ajmms.20241403.42
Received: Mar. 1, 2024; Accepted: Mar. 20, 2024; Published: Mar. 22, 2024

Clinical and Morphological Condition of Strictures of the Anal Canal
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLInagamova Makhliyo Khojiakbarovna1, Baymakov Sayfiddin Risbaevich1, Adilbekova Dilorom Bakhtiyarovna2
1Department of General Surgery and Military Field Surgery, Tashkent State Dental Institute, 103 Tarakkiyot Street, Tashkent, Uzbekistan
2Department of Anatomy and Clinical Anatomy, Tashkent Medical Academy, Forobiy 2, Tashkent, Uzbekistan
Correspondence to: Inagamova Makhliyo Khojiakbarovna, Department of General Surgery and Military Field Surgery, Tashkent State Dental Institute, 103 Tarakkiyot Street, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Anal stricture disease occupies a leading position among complications after surgical operations in the perianal areas. The main causes of anal and rectal strictures are surgical trauma, inflammatory bowel diseases, infections and fibrosis, sexually transmitted diseases, tuberculosis, and chronic laxative abuse. Morphologically, with strictures around the anus, scar growths, deformation of the walls of venous vessels, and inflammatory infiltrates in the interstitial tissue are revealed. The morphological picture of a scar lesion in the anorectal area makes it possible to assess the maturity of the pathological connective tissue and determine the treatment tactics for this process.
Keywords: Anal canal, Strictures, Morphological condition, Diagnosis
Cite this paper: Inagamova Makhliyo Khojiakbarovna, Baymakov Sayfiddin Risbaevich, Adilbekova Dilorom Bakhtiyarovna, Clinical and Morphological Condition of Strictures of the Anal Canal, American Journal of Medicine and Medical Sciences, Vol. 14 No. 3, 2024, pp. 739-742. doi: 10.5923/j.ajmms.20241403.42.
Article Outline
1. Introduction
- Postoperative anal stricture is a serious disease caused by pathological narrowing of the anus resulting from excision of the perianal skin and anal mucosa, which were replaced by connective tissue [3,5,8,11,12]. The most common cause of postoperative anal strictures is hemorrhoidectomy, ranging from 1.5% to 3.8%. The incidence of the disease, according to various authors, has fluctuated over several decades in the range of 2-9% of all patients operated on for benign diseases of the rectum [1,4,6,10]. V.V. Balitsky et al. (2021) summarizing the experience of treating postoperative summarizing the experience of treating postoperative anal canal stenoses, note that strictures of the anal canal after hemorrhoidectomy occur in 5-10% of cases. There are various approaches of specialists to this problem. These are conservative methods, including adherence to a slag-free diet, the use of laxatives, enemas, and various bougienage techniques. Treatment of postoperative anal canal stenosis remains a difficult problem in modern surgery.
2. Aim of the Study
- To study the basics of clinical and morphological features of various strictures of the anal canal and rectum.
3. Materials and Methods
- For 2020-2023 30 patients with cicatricial strictures of the anal canal were operated on in the department of coloproctology. The main cause of cicatricial stenosis was surgery on the rectum and anal canal. The average age of patients was 28-51 years. There were 23 women, 7 men. Postoperative strictures looked like dense ring-shaped formations measuring 0.5-1.5 cm in diameter. Materials obtained from dense formations of the anal canal were fixed in Carnoy's fluid and in a 10% solution of neutral formalin. After appropriate processing, the materials were embedded in paraffin and sections with a thickness of 4-6 microns were prepared from them. Afterwards, the sections were stained with hematoxylin-eosin and Van Gieson. Finished microspecimens were studied in MBS-9 microscopes.
4. Results and Discussions
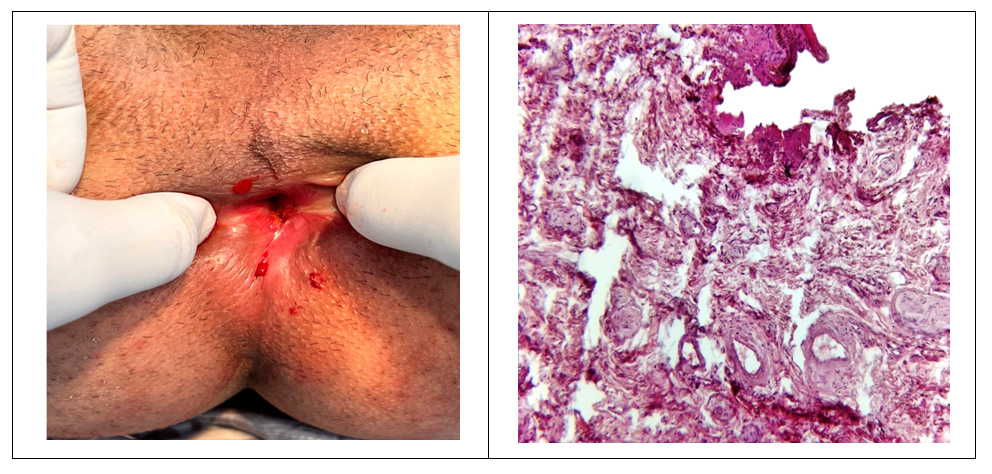
- Our research data showed that the narrowing may be the result of a true stricture (organic) or functional muscle stenosis. With organic stenosis, the normal epithelial lining of the anal canal is replaced to varying degrees by dense scar tissue, which causes morphological changes in the anal canal with a subsequent decrease in its function and leads to difficult and painful defecation. The stenotic segment may be located in the proximal or distal part of the anal canal, but often the pathologically altered tissues are located diffusely and circularly, involving the entire anal canal. The causes of anal strictures may be other operations on the anal canal, which require wide excision of the affected tissue, removal of the perianal skin and mucous membrane of the anal canal, trauma, inflammatory bowel diseases (in particular Crohn's disease), radiation therapy (for example, with uterine cancer, prostate cancer), sexually transmitted diseases (Nicola-Favre disease), tuberculosis and chronic laxative abuse, sepsis, ischemia due to occlusion of the inferior mesenteric artery or superior rectal artery, AIDS, infections, fibrosis and spasm of the anal sphincter, perineal trauma, chronic inflammatory process in the rectum, chemical burn of the anal canal and rectum.Wide excision of the mucous membrane of the anal canal, without leaving adequate mucocutaneous bridges, leads to the formation of scars, the occurrence and progression of postoperative stenosis of the anal canal. Radical operations performed against the background of ongoing bleeding and severe anemia may be accompanied by the formation of rough scars in the anal canal.In the natural anatomical configuration in healthy people, the anal canal is an inverted tube, where its diameter is smaller than the diameter of the anal verge. In this example, it is important to distinguish between acute anal stenosis and chronic anal stenosis. Acute anal stenosis (spasm) is defined by a strong and sudden narrowing with constant pain (anal fissure). Morphologically, infiltration and swelling and proliferation of coarse fibrous structures in the tissue structures of the anal canal are observed (Fig. 1). This stenosis is reversible. In this case, the anorectal meatus becomes cylindrical.
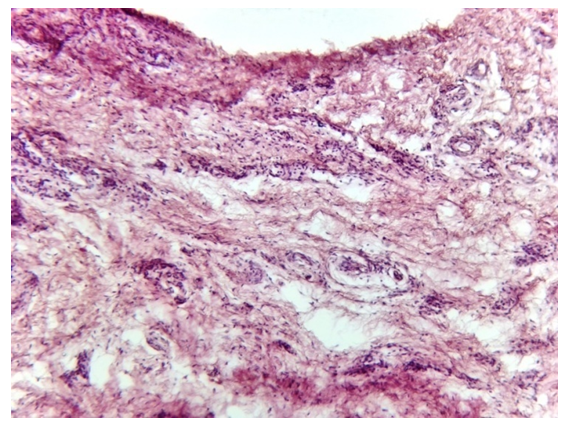 | Figure 1. Acute stenosis of the anal canal. Infiltration and swelling, proliferation of coarse fibrous structures in the tissue structures of the anal canal. G.E. 10×10 |
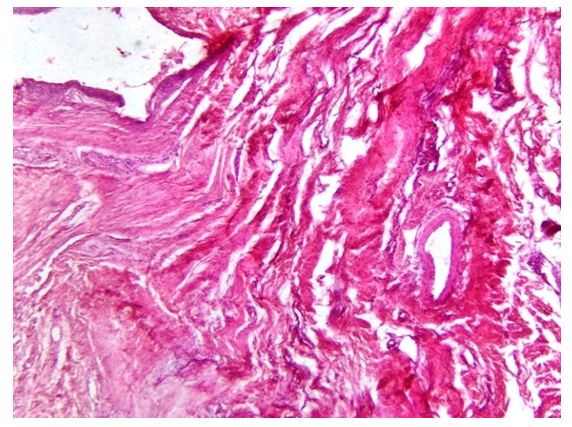 | Figure 2. Chronic anal stenosis. There are scar growths around the anus, the walls of the venous vessels are deformed, inflammatory infiltrates in the interstitial tissue. G.E. 10×10 |
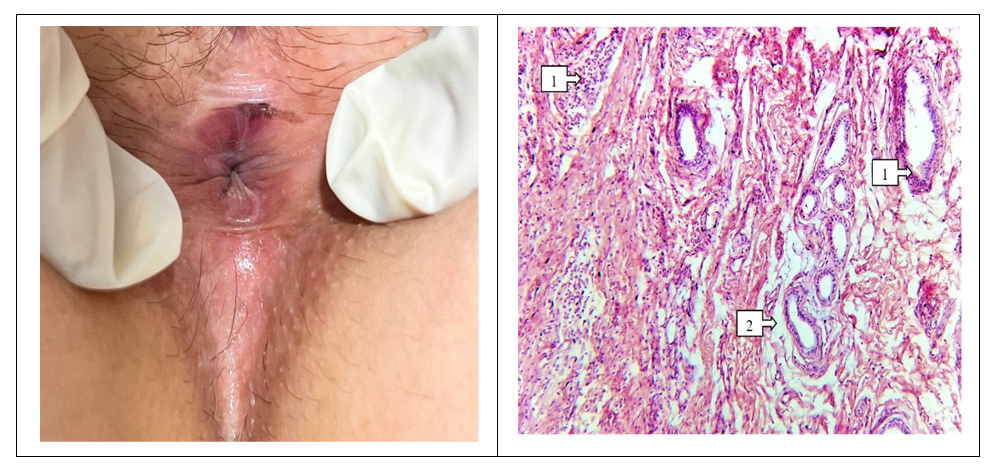 | Figure 3. Stricture of the anal canal is a stage of compensation. Metaplasia of glandular structures and sinusoids (1); chaotically located fibromatous fibrous structures are visible (2). Muscular components are not detected. Coloring by G.E. 10 ×10 |
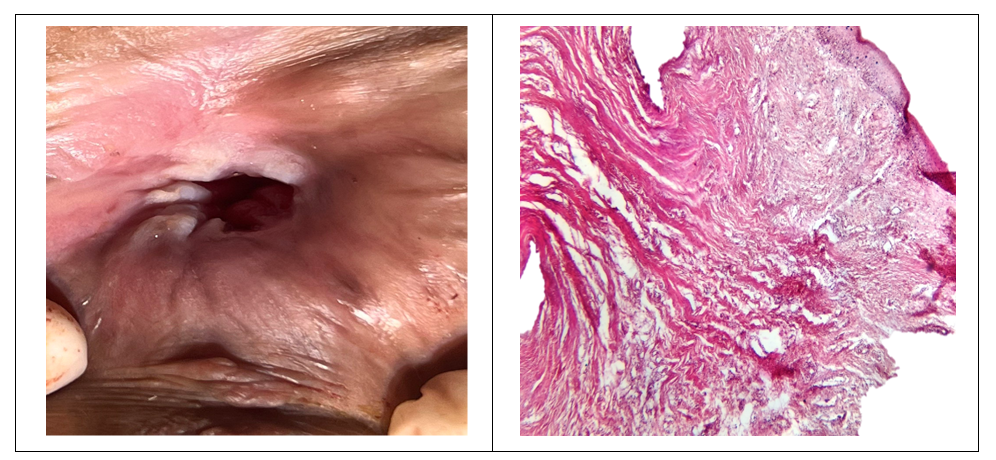 | Figure 4. Stricture of the anal canal is the stage of subcompensation. The stricture consists of coarse fibrous tissue (1), the scars protrude towards the anus, vascular formations are not detected (2). Coloring by G.E. 4×10 |
 | Figure 5. Stricture of the anal canal - stage of decompensation. Hyalinosis of the walls of blood vessels and obliteration of blood vessels around the anus are detected (1), infiltration of the interstitial tissue is noted (2), and destruction occurs in the fibrous structures (3). Coloring by G.E. 40 ×10 |
5. Conclusions
- 1. The main causes of strictures of the anal canal and rectum are surgical trauma, inflammatory bowel diseases, infections and fibrosis, sexually transmitted diseases, tuberculosis, and chronic laxative abuse.2. Morphologically, with strictures around the anus, scar growths, deformation of the wall of venous vessels, inflammatory infiltrates in the interstitial tissue are revealed.3. The morphological picture of a scar lesion in the anorectal area allows us to assess the maturity of the pathological connective tissue and determine the treatment tactics for this process.