-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(3): 708-712
doi:10.5923/j.ajmms.20241403.37
Received: Feb. 25, 2024; Accepted: Mar. 11, 2024; Published: Mar. 14, 2024

A New Approach to the Prevention of Acute Pancreatitis after Retrograde Endoscopic Manipulations
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLM. S. Khakimov, Sh. E. Ashurov, J. Kh. Kushiev, J. R. Asatullaev, B. M. Sobirov, J. Sh. Abdukarimov
Tashkent Medical Academy, Tashkent, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of the study was to identify risk factors for the development of acute pancreatitis during retrograde interventions and to create a prognostic scale for improving the treatment results of acute postmanipulatory pancreatitis. Background. Despite the improvement of medical technologies and the development of the pharmaceutical industry, the incidence of acute pancreatitis after retrograde endoscopic procedures remains in the range of 3.0-12.0%, and mortality reaches up to 15%. Today, retrograde endoscopic interventions play a huge role in the diagnostics and treatment of obstructive jaundice of various origins. At benign genesis of mechanical jaundice in 80-90% of cases retrograde endoscopic interventions allow to diagnose the cause of the disease and to perform adequate decompression of the biliary system. Material and Methods. The examination and treatment results of 396 patients treated at the multidisciplinary clinic of Tashkent Medical Academy for the period from 2015 to 2022 who underwent retrograde interventions were analyzed. The age of the patients ranged from 18 to 85 years. There were 220 females and 176 males. Results. The treatment results of 396 patients with signs of mechanical jaundice of benign genesis were presented. We used the scale developed for predicting the development of acute postmanipulatory pancreatitis. It allowed to perform a differentiated approach to Retrograde Endoscopic Intervention taking into account the risk assessment of acute pancreatitis development and contributed to a 3-fold decrease in the incidence of postmanipulation complications. Conclusion. Application of the developed prognostic scale of acute pancreatitis at retrograde endoscopic manipulations in treatment of mechanical jaundice of benign genesis allowed to reduce the frequency of acute pancreatitis development from 13,3% to 3,5%, and the frequency of lethality - from 3,6% to 1,0%.
Keywords: Mechanical jaundice, Retrograde endoscopic interventions, Cholangiopancreatography, Pancreatitis
Cite this paper: M. S. Khakimov, Sh. E. Ashurov, J. Kh. Kushiev, J. R. Asatullaev, B. M. Sobirov, J. Sh. Abdukarimov, A New Approach to the Prevention of Acute Pancreatitis after Retrograde Endoscopic Manipulations, American Journal of Medicine and Medical Sciences, Vol. 14 No. 3, 2024, pp. 708-712. doi: 10.5923/j.ajmms.20241403.37.
Article Outline
1. Introduction
- Despite the improvement of medical technologies and the development of the pharmaceutical industry, the incidence of acute pancreatitis (AP) after retrograde endoscopic procedures remains in the range of 3.0-12.0%, and mortality reaches up to 15% [1-7]. Today retrograde endoscopic interventions play a huge role in the diagnostics and treatment of mechanical jaundice (MJ) of various genesis. In benign genesis of MJ in 80-90% of cases retrograde endoscopic interventions allow to diagnose the cause of the disease and perform adequate decompression of the biliary system [1-4]. The main requirements for modern treatment methods are high clinical efficiency with low injury and low rates of postoperative complications and lethality [1,8,3,9-12]. Retrograde endoscopic interventions fulfill the above criteria, especially in the treatment of mechanical jaundice of benign genesis [13,10]. These interventions have a certain advantage - the ability to move from the diagnostic stage to the therapeutic stage; if necessary, to ensure adequate internal bile drainage and complete sanitation of the biliary tract, endoscopic papillosphincterotomy is performed, which is an effective method in the treatment of choledocholithiasis and stenosis of the major duodenal papilla (MDP) [1,3-4,9,13,7,11]. After performing therapeutic procedures, the incidence of AC development is 3.0-12.0%, and mortality reaches up to 15.0% [1-2,8,3,10,12].The diagnostic and therapeutic effectiveness of retrograde endobiliary interventions is 85-95.0% of cases, which is directly related to the shape and location of the MDP, the length of the longitudinal fold, previous operations on the gastrointestinal tract, the nature and cause of MJ, as well as the number and size of stones, the severity of cholangitis, experience of the surgeon [1-2,4,9,7,11-12]. All of the above criteria lead to one or another technical difficulty during each stage: visualization and cannulation of MDP, papillosphincterotomy, lithotripsy or stone removal. It should be noted that the highest number of AP is observed in those patients who have technical difficulties during retrograde endoscopic interventions [1-2,4,6,12].Acute post-manipulation pancreatitis is an acute inflammation of the pancreas, usually developing during retrograde endoscopic interventions as a result of repeated cannulation of the Wirsung duct, reflux of bile into the ducts of the gland, injury to the mucous membrane of the pancreatic duct, entry of a contrast agent into the ducts of the gland, improper use of the electrocoagulation mode, dissection of the papilla and sphincter in the wrong direction with insufficient visualization, when attempting to remove large stones through the sphincterotomy opening [1-4].Many authors argue that adherence to preventive measures for the development of AP after retrograde manipulation is sufficient and there is no need to predict such a complication [4,7,11]. But, unfortunately, even in patients who underwent preventive measures before performing retrograde interventions, there was no significant reduction in the incidence of pancreatitis [11-12].Currently, there are no widely accepted prognostic scales for the development of AP. The aim of the study was to identify risk factors for the development of acute pancreatitis during retrograde interventions and to create a prognostic scale for improving the treatment results of acute postmanipulatory pancreatitis.
2. Material and Methods
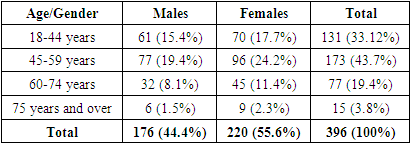
- The examination and treatment results of 396 patients treated at the multidisciplinary clinic of Tashkent Medical Academy for the period from 2015 to 2022 who underwent retrograde interventions were analyzed. The age of the patients ranged from 18 to 85 years. There were 220 females and 176 males (Tab. 1).
|
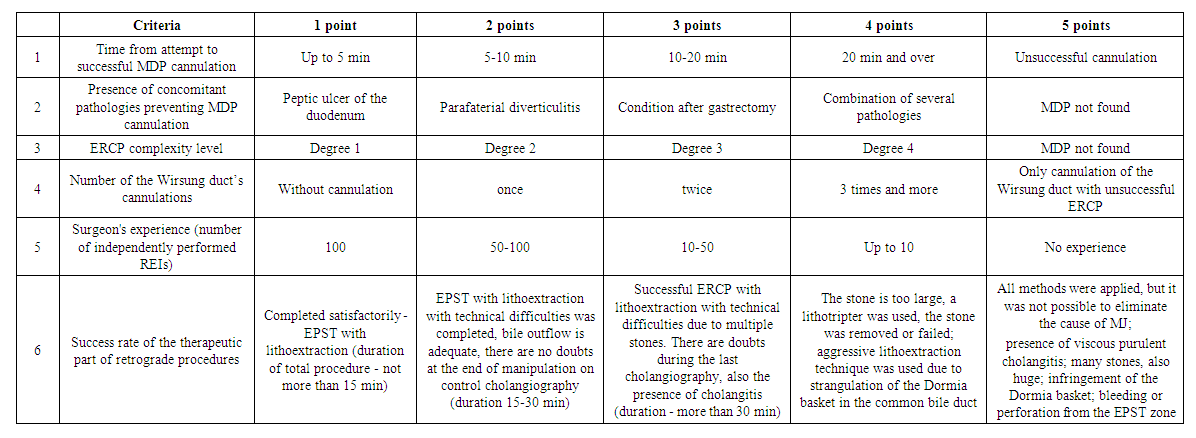 | Table 2. AP prediction scale after retrograde interventions in the treatment of mechanical jaundice |
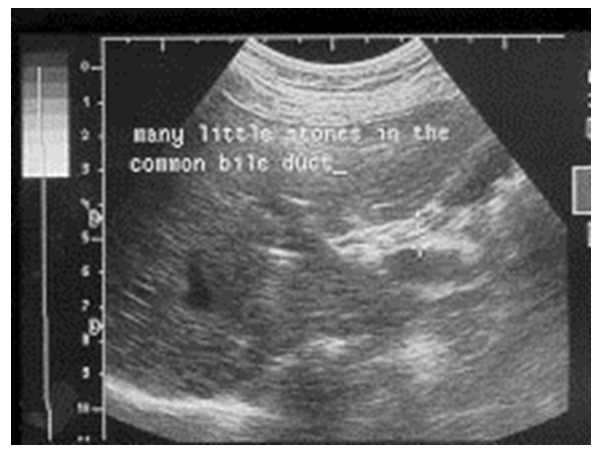 | Figure 1. Ultrasound examination of choledocholithiasis |
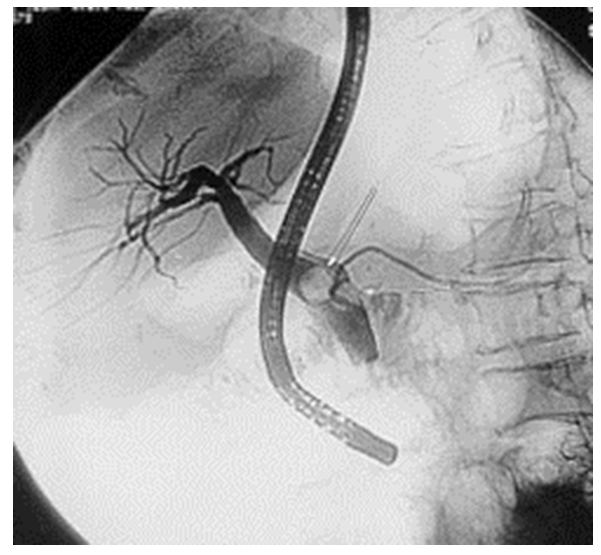 | Figure 2. Retrograde cholangiopancreatography for choledocholithiasis |
3. Results
- We analyzed the incidence of AP development after retrograde procedures according to the results of the prediction scale. Patients who had the development of other complications after retrograde interventions were excluded from the study. Taking into account the fact that a retrospective analysis was conducted in the control group, patients were empirically ranked by 10 points into three groups to determine the risk of developing acute pancreatitis. The maximum number of points on the scale we offer was 30. 127 (64.8%) from 196 patients in the control group made up group 1 (the number of points was up to 10), 38 (19.4%) patients were included in group 2 (11-20 points) and the remaining 31 (15.8%) – in group 3 (21 points and above). All patients in this group underwent retrograde endoscopic interventions to decompress the biliary system.In group 1, 2 (1.6%) cases showed signs of acute edematous pancreatitis. A positive clinical result was achieved against the background of conservative therapy.AP developed in 9 (23.7%) cases of group 2. In 3 of them the development of pancreonecrosis with subsequent infection of the focus required surgical interventions. In other observations acute pancreatitis was treated by conservative measures. No lethal outcomes were noted. In group 3, AP was developed in 15 (48.4%) patients: 4 had edematous form, 3 had sterile pancreonecrosis, and 8 had infected pancreonecrosis (those patients were performed surgical intervention).There was a lethal outcome in 7 (3.6%) cases against the background of progression of pancreatogenic toxemia and development of multiorgan failure.In the main group, according to our proposed AP prognosis scale, group 1 included 162 (81.0%) patients, group 2 included 21 (10.5%) patients, and group 3 included 17 (8.5%) patients. The treatment tactics depended on the scores in this group. If more than 15 points were accumulated during retrograde manipulations, the study was terminated and antegrade endobiliary interventions were performed. In group 1 AP was developed in 4 (2.5%) cases, in group 2 - in 1 (4.8%) case, in group 3 AP development was noted in 1 (11.8%) patient. Lethal outcome was noted only in 2 (1.0%) cases.
4. Discussion
- Analysis of unsatisfactory results in the control group showed that their reasons were attempts to complete the treatment stage as much as possible in the prescribed manner, regardless of the technical difficulties of retrograde interventions and the presence of a high risk of developing AP. In addition, those patients who underwent repeated attempts at ERCG were prescribed alternative treatment methods only after 1-2 days, which could provoke the development of severe forms of acute pancreatitis.According to a number of researchers (Andriulli A. (2007); Arata S. (2010); Masci E. (2003); Saritas U. (2011)) there is no consensus on the reasons for the development of acute post-manipulation pancreatitis [7,10-12]. Several major mechanisms of its development are considered: hydrostatic, chemical, allergic, enzymatic, infectious, thermal, mechanical [12]. Despite these data, in our opinion, one of the main causes contributing to the development of acute post-manipulative pancreatitis is a mechanical factor.Regardless of the trigger, injury to the pancreas leads to an autoimmune attack followed by the manifestation of acute pancreatitis. Another leading cause of acute post-manipulation pancreatitis may be an increase in pressure in the pancreatic ducts during cholangiopancreatography or due to obstructed outflow of secretions due to edema or injury to the orifice of the duct [1-2]. The reflux of a contrast agent into the Wirsung duct often becomes a trigger for acute pancreatitis.In this regard, preventive measures taken should be aimed at one or more factors that can prevent complications of retrograde procedures. These include prevention of outflow disturbances from the main duct of the pancreas, prevention of inflammation, reduction of spasm of the Oddi sphincter and pancreatic secretion [9]. Taking into account the above factors, we have developed an AP prognosis scale, which allows to prevent the development of complications of retrograde interventions by justifying the feasibility of alternative methods of the biliary system decompression, which made it possible to reduce the incidence of AP after retrograde interventions by almost 2.5-3 times.
5. Conclusions
- The most common factors influencing the development of acute pancreatitis during retrograde endobiliary interventions are the time from the moment of attempt to successful MDP cannulation; the presence of concomitant pathologies that prevent MDP cannulation; the degree of complexity of ERCPG; the number of cannulations of the Wirsung duct; the number of independently performed REI; the degree of success of the therapeutic part of retrograde procedures.The use of the developed prognostic scale of acute pancreatitis at retrograde endoscopic manipulations in treatment of mechanical jaundice of benign genesis allowed to reduce the number of acute pancreatitis from 13.3% to 3.5%, and the incidence of lethality due to AP -from 3.6% to 1.0%.
Conflict of Interests
- The authors declare no conflict of interest. This study does not include the involvement of any budgetary, grant or other funds. The article is published for the first time and is part of a scientific work.
ACKNOWLEDGEMENTS
- The authors express their gratitude to the management of the multidisciplinary clinic of Tashkent Medical Academy for the material provided for our study.