-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(3): 649-656
doi:10.5923/j.ajmms.20241403.24
Received: Feb. 12, 2024; Accepted: Mar. 2, 2024; Published: Mar. 7, 2024

Assessment of Functional Disorders Using the GMFCS and MACS Classification in Patients with Cerebral Palsy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNasirova Iroda Rovshan Qizi, Ziyakhodzhayeva Latofat Uchkunovna
Department of Neurology, Pediatric Neurology and Medical Genetics, Tashkent Pediatric Medical Institute, Tashkent, Republic of Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

At the present stage of the development of medical science, cerebral palsy is considered a polyethological disease that includes various clinical variants of the course and is characterized by a diverse pattern of manifestations. In this article, to assess the ability of patients with cerebral palsy to walk independently and self-care, we conducted a study of the level of development of large motor functions in these children.
Keywords: Cerebral palsy, GMFCS, Motor disorders, Functional capabilities
Cite this paper: Nasirova Iroda Rovshan Qizi, Ziyakhodzhayeva Latofat Uchkunovna, Assessment of Functional Disorders Using the GMFCS and MACS Classification in Patients with Cerebral Palsy, American Journal of Medicine and Medical Sciences, Vol. 14 No. 3, 2024, pp. 649-656. doi: 10.5923/j.ajmms.20241403.24.
Article Outline
1. Introduction
- Cerebral palsy is defined as persistent disorders of the formation of motor skills and maintaining posture, leading to restriction of optimal functioning and movement disorders due to non-progressive damage and/or abnormality of the brain forming in the fetus or newborn child [1,10]. At the present stage of the development of medical science, cerebral palsy is considered a polyethological disease that includes various clinical variants of the course and is characterized by a diverse pattern of manifestations [3,9].Leading scientists from all over the world are involved in the study of this serious disease. Despite this, the specific causes of cerebral palsy are still not fully understood, therefore, there is a lack of clarity in the prevention of this severe pathology. In most cases, there are several reasons for the occurrence of cerebral palsy. Adverse factors are found both during pregnancy and directly during childbirth, but which of them play the most significant role is still unknown [4,14,15,16].Thus, cerebral palsy is a symptom complex with a large clinical polymorphism as a result of perinatal, mainly antenatal, brain damage [14]. But questions about the true causes and characteristics of the course of this disease still do not have unambiguous answers [8,11].It is believed that the diagnosis of cerebral palsy can be determined by the end of the first year of a child's life. By this period, a delay in motor development can already be clearly formed, a core arises for the development of a pathological motor stereotype in the patient, and it becomes obvious that the identified violations are not compensable. Naturally, it is very important to exclude other pathologies of the central nervous system, which can display a similar clinical picture of motor disorders [5,7].To assess the functional abilities of children with cerebral palsy, large motor function assessment systems (GMFCS), the Manual Skills Classification System (MACS), and the communication Skills Assessment System (CFCS) are currently used.The use of GMFCS is possible in children with cerebral palsy from the age of 1.5 years. The advantage of this classification system is the ability to identify not only the severity of motor disorders, but also to predict the formation of global motor functions of a child during his or her lifetime [2,12,13]. Gait analysis using GMFCS is used to objectively assess the level of motor disorders in children with cerebral palsy, based on their functionality, the need for auxiliary devices (walkers, support frames, crutches, sticks, strollers) and movement capabilities, and to a lesser extent on the quality of the child's movements [13].This classification was developed by the staff of the Canadian McMaster University, translated into many languages of the world and is currently a generally accepted international standard. According to the GMFCS classification, all patients with cerebral palsy are divided according to their motor abilities into five levels:1) level "I" corresponds to children who can walk without restrictions, but cannot cope with more complex motor tasks; 2) children can walk independently with a slight restriction and cope with the simplest motor tasks; 3) children move satisfactorily with the help of additional support, take several independent steps; 4) children can hardly move with the help of additional support, but do not require constant support from an accompanying person; 5) level "5" corresponds to patients with very limited opportunities for independent movement, even with auxiliary equipment and weak control of the position of the trunk and head.In order to determine the function of the upper extremities in patients with cerebral palsy, all patients were assessed for their manual skills according to the MACS classification system (Manual Ability Classification System). The MACS functional class I determines the patient's ability to use the upper limb to its full extent, that is, the function is not impaired. Patients with class II manual skills in most cases effectively use the upper limb, but some actions are performed more slowly or less efficiently than patients with class I MACS. The III functional class of MACS defines the difficulty of the functional capabilities of the upper limb. The patient needs to prepare for action or is forced to adapt it to his abilities. Functional class IV is typical for patients with limited upper limb function, and its use is possible only in an adapted situation. The V class of MACS defines a complete violation of the function of the upper limb, regardless of the situation created. The purpose of the study. To assess functional disability in patients with cerebral palsy using the classification of gross motor Functions (GMFCS) and manual skills (MACS).
2. Materials and Research Methods
- The research was conducted at the Department of Neurology with Pediatric Neurology of TashPMI, at the clinic of LLC "REACENTER-TASHKENT" and the children's Neuropsychiatric hospital named after U.K. Kurbanov. The work is based on the analysis of 134 patients with motor disorders. The age of the children ranged from 3 years old to 15 years old. To assess the ability of patients with cerebral palsy to walk independently and self-care, we conducted a study of the level of development of large motor functions (GMFCS) and manual skills (MACS) in these children.
3. Results and Discussions
- The class of development of large motor functions according to the classification of large motor functions (GMFCS) was identified. The first functional class, which corresponded to walking without any restrictions, was determined in 71 sick children (53±0.25%), the 2nd functional class, characterized by the ability of patients to walk with restrictions, was noted in 36 patients (27±0.2%), the 3rd functional class according to GMFCS (walking with manual devices) was observed in 17 patients (13±0.11%), 4th and 5th classes of GMFCS, this is the ability of patients to move using motorized means and complete dependence on others were determined in 7 (5±0.05%) and 3 (2±0.02%) cases, respectively (Figure 1).
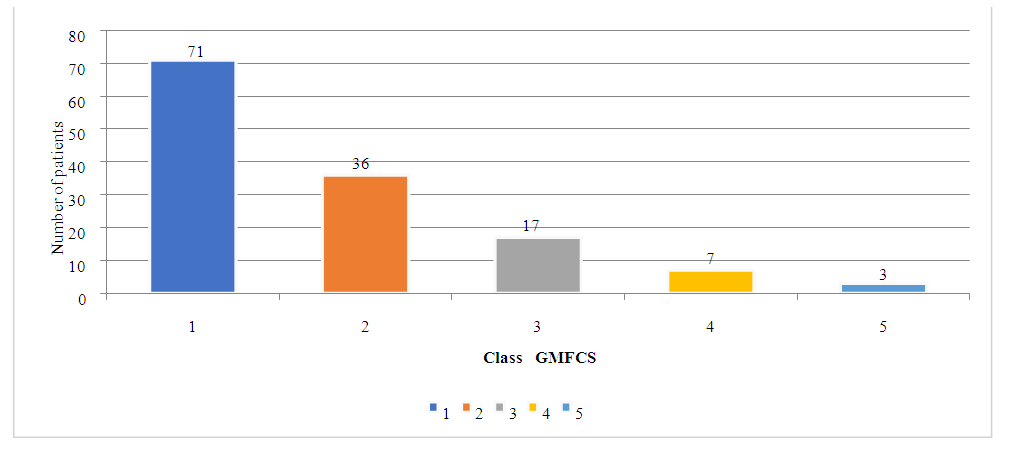 | Figure 1. Distribution of patients (number of patients) by classes of major motor functions (GMFCS) |
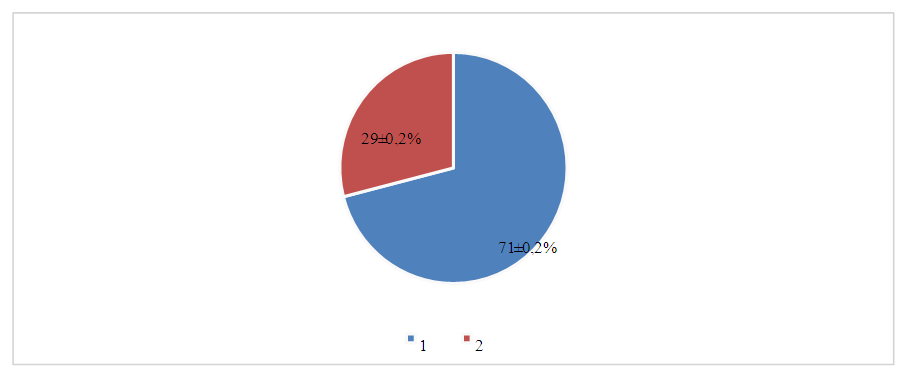
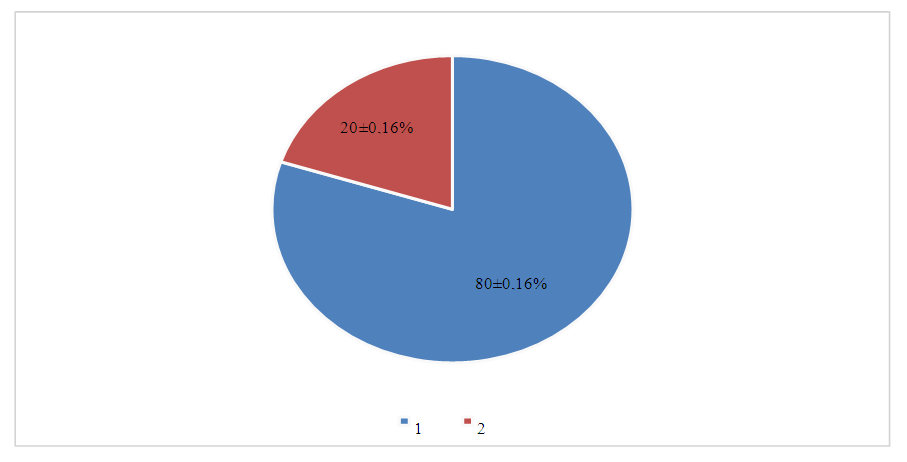
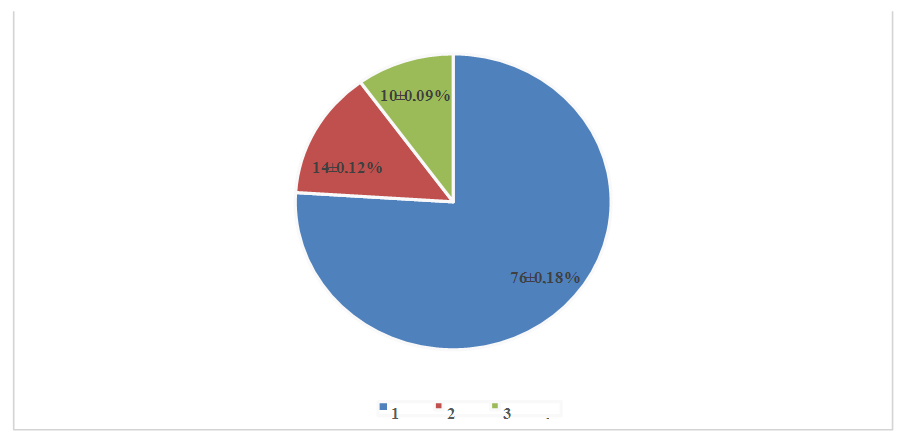 | Figure 2. Distribution of children with bilateral spastic cerebral palsy by functional classes of large motor functions |
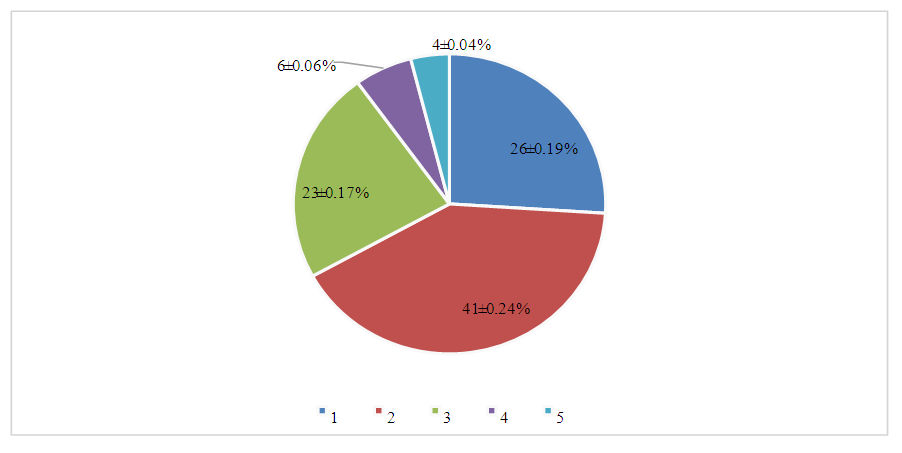
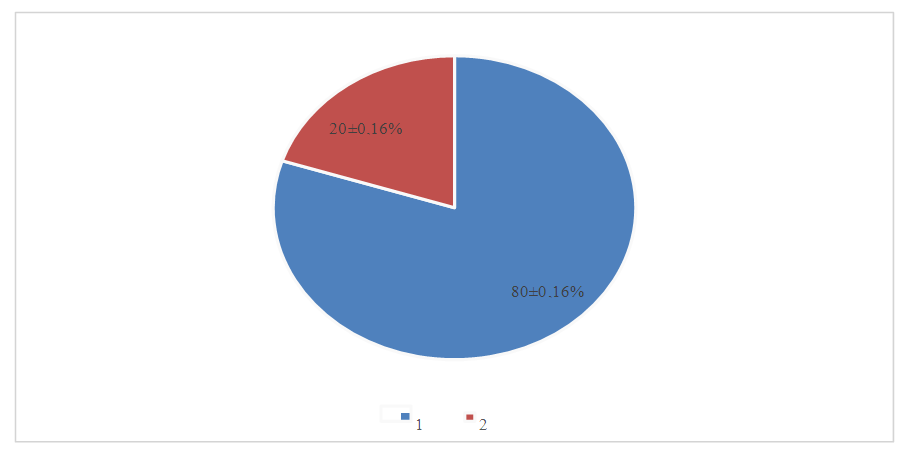 | Figure 3. Distribution of children with unilateral spastic cerebral palsy by functional classes of large motor functions |
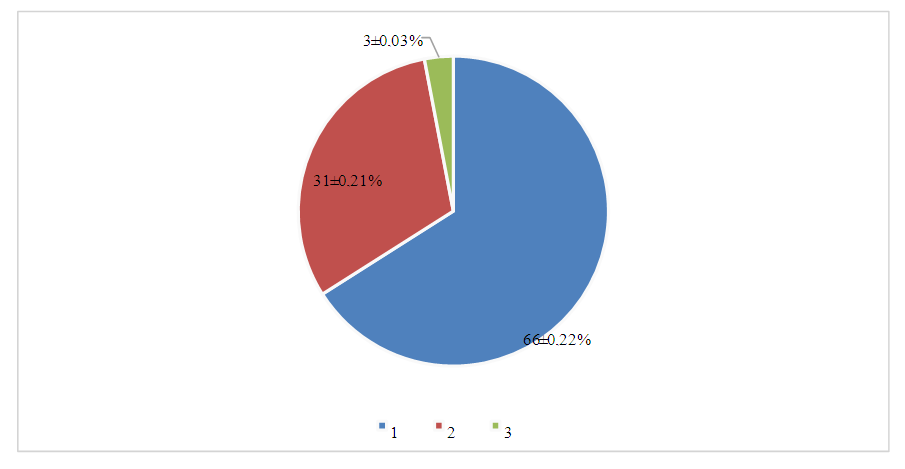
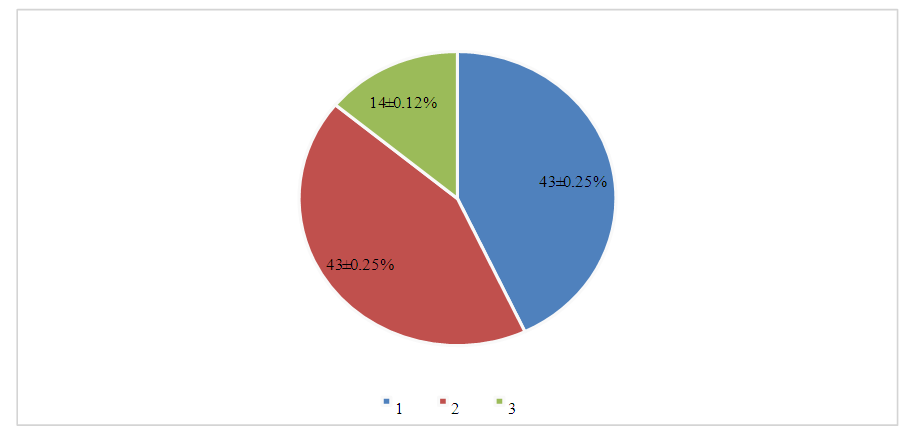
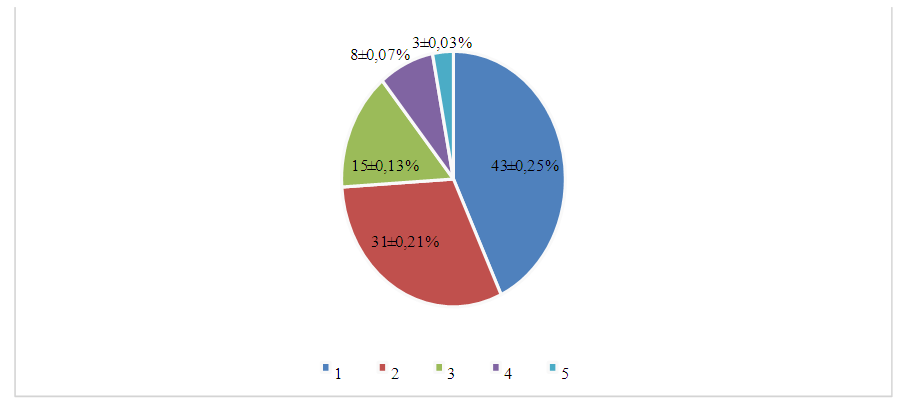 | Figure 4. Distribution of children with a mixed variant of cerebral palsy by functional classes of large motor functions |
 | Figure 5. Distribution of children with dyskinetic variant of cerebral palsy by functional classes of large motor functions |
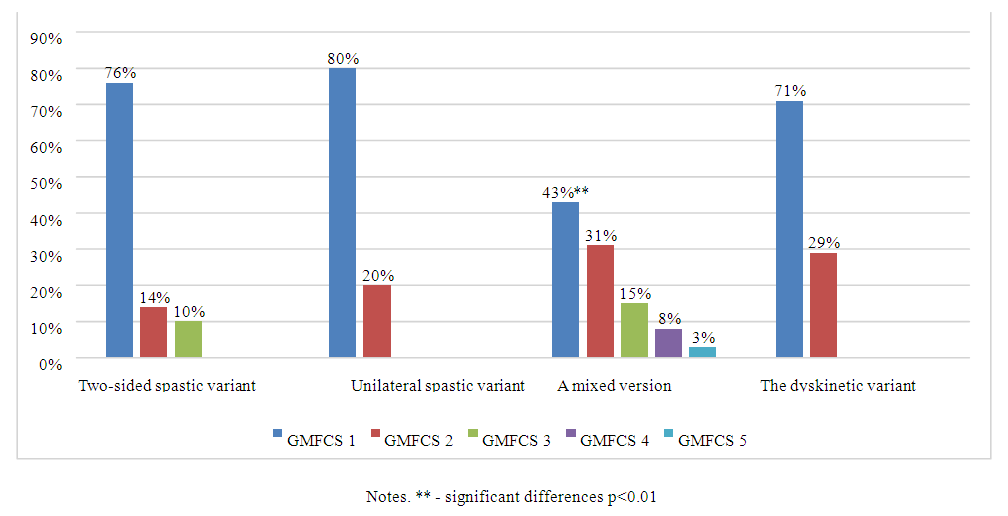 | Figure 6. Distribution of children with different clinical variants of cerebral palsy by functional classes of large motor functions |
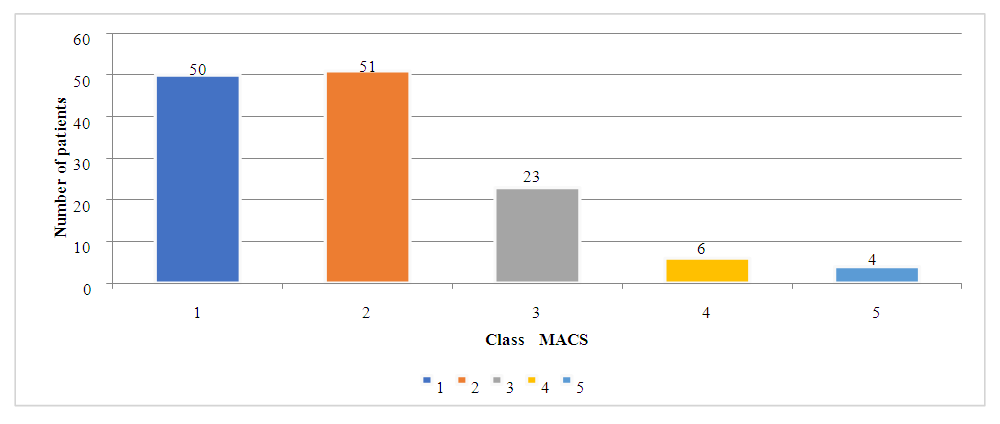 | Figure 7. Distribution of children with cerebral palsy (number of patients) by classes of manual abilities (MACS) |
 | Figure 8. Distribution of children with bilateral spastic cerebral palsy by functional classes of manual skills |
 | Figure 9. Distribution of children with unilateral spastic cerebral palsy by functional classes of manual skills |
 | Figure 10. Distribution of children with mixed cerebral palsy by functional classes of manual skills |
 | Figure 11. Distribution of children with dyskinetic cerebral palsy by functional classes of manual skills |
 | Figure 12. Distribution of children with different clinical variants of cerebral palsy by functional classes of manual skills |
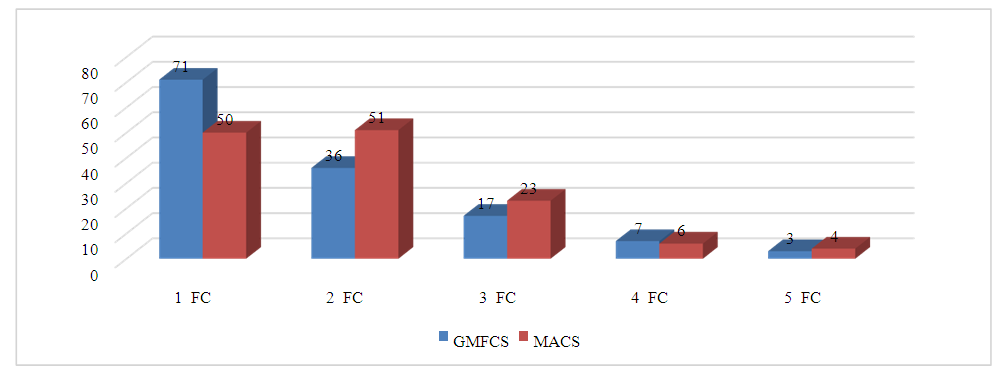 | Figure 13. Distribution of GMFCS and MACS classes across the entire group of examined patients |
4. Conclusions
- 1. The frequent occurrence of the first two functional classes according to GMFCS and MACS in the same patients is explained by the fact that the study was dominated by outpatient patients who, in addition to the possibility of independent or assisted walking, had satisfactory manual skills, combined to ensure their adaptation to everyday life. 2. Thus, as the GMFCS class increases, there is also a deterioration in the functionality of the upper extremities according to MACS.3. The most pronounced disorders of large motor functions and manual skills were noted with a mixed form of cerebral palsy, which indicates the presence of various types of motor disorders in their clinical picture and allows us to consider this variant of the course of the disease unfavorable.