Nadyrkhanova N. S., Abdullazhonova K. N.
Republican Specialized Scientific and Practical Medical Center for Maternal and Child Health, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
In analyses of maternal mortality, cardiovascular disease has a leading place. To study the course of pregnancy and delivery made a retrospective analysis of 204 histories of pregnant women with myocarditis.
Keywords:
Pregnancy, Myocarditis, Cardiovascular disease
Cite this paper: Nadyrkhanova N. S., Abdullazhonova K. N., Retrospective Analysis of the Course of Pregnancy and Labour in Pregnant Women with Myocarditis, American Journal of Medicine and Medical Sciences, Vol. 14 No. 3, 2024, pp. 640-642. doi: 10.5923/j.ajmms.20241403.21.
1. Introduction
Cardiovascular disease is said to occur in 1-4% of all pregnancies and represents a high risk of perinatal complications, also accounting for up to 10% of maternal mortality [1,5]. In this case, myocarditis in pregnancy is rarely observed, but when cardiomyopathy develops, it is the most threatening and life-threatening condition among all cardiovascular complications [2,5,6]. One of the most important issues of modern gynaecology and cardiology, underlying the prevention of sudden death and other complications (prolonged persistent left ventricular dysfunction, dilated cardiomyopathy, pulmonary embolism) in myocarditis in pregnant women, is the prediction of their development, clarification of the role of new predictors of unfavourable outcome of the disease after delivery [1,3,4]. In the world practice at the present time, the most urgent questions are the peculiarities of a specific approach to the verification of myocarditis for the purpose of adequate management of delivery and prevention of heart failure after delivery [2,5,9]. Numerous scientific studies continue to investigate the direct proportional effect of early detection of myocarditis in pregnant women with the inclusion of its trimester-associated conservative treatment on the quality of life of both mother and foetus in the perinatal period, including a reduction in the incidence of maternal mortality [7,8].Purpose of the study. Analysis of pregnancy and labour in pregnant women with myocarditis.
2. Materials and Methods of the Research
We retrospectively analysed 3012 birth histories of births that occurred at RSSPMCMCH in 2020-2021. The results of the retrospective analysis showed that among the general population of pregnant women admitted for delivery at RSSPMCMCH 13.7% of women had cardiovascular disease (CVD). The analysis showed that among the nosological forms of CVD in pregnant women, myocarditis (postmyocardial cardiosclerosis (PMCS)) was the most frequent, 49.4%.
3. Results of the Research
In retrospective analyses, in pregnant women with myocarditis, 53.4% of cases were women in active reproductive age and 7.8% of cases were women above 35 years of age.Table 1. Age-related aspects of pregnant women with myocarditis
 |
| |
|
The study of parities in the main group showed first-pregnant women were – 29% and multiparous (3 or more births) - 25%, and repeat-pregnant women (repeat births) - 49%) and repeat-pregnant women (first births) - 6%. (table 2).Table 2. Pregnancy parity by retrospective analysis
 |
| |
|
The most common complaints of pregnant women with myocarditis were dyspnoea 56 (27.5%), general weakness 62 (30.4%) palpitations 59 (29%), in rare cases there was pain in the heart area 18 (8%). Single complaints were present in 25% of pregnant women, while the rest had a combination of several complaints (figure 1).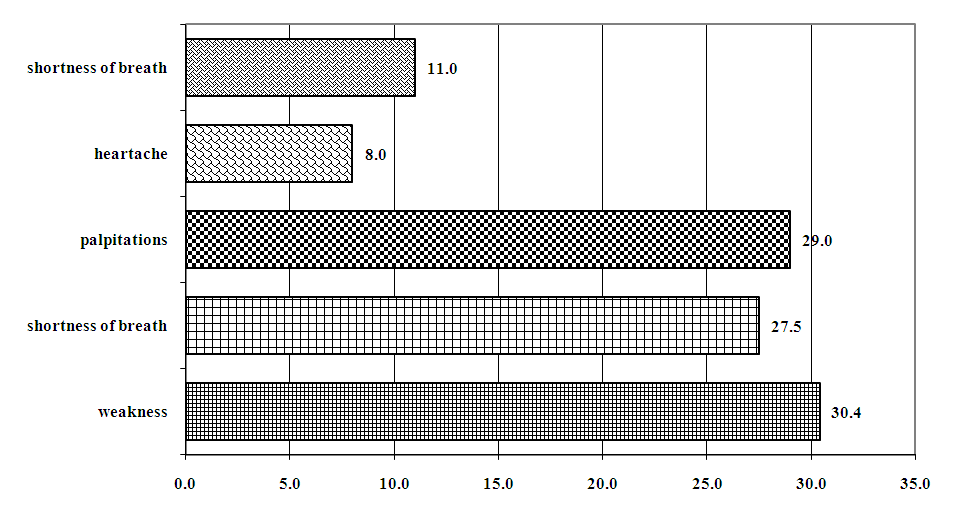 | Figure 1. Structure of subjective complaints of pregnant women with myocarditis |
In pregnant women with myocarditis, the labor process was complicated: 7 (3.4%) had an anomaly of labor, 4 (2.0%) women had rapid labor, and 5% had hemorrhage. A likely factor in the development of perinatal complications in pregnant women with myocarditis was a pathologic preliminarian period, which accounted for 9.3% of cases (asphyxia of the 1st and 2nd degrees).The course of the postpartum period in laboring women with myocarditis was complicated by uterine subinvolution in 8 (6.4%), lactostasis in 8 (4.0%) and 25.5% with circulatory disorders. Currently, despite numerous studies in cardiology, the choice of method and timing of delivery in pregnant women with myocarditis is not an easy task for obstetricians and gynecologists. Today, the frequency of abdominal delivery and the proportion of pregnant women with uterine scarring are increasing. Retrospective analysis of the method of delivery in pregnant women with myocarditis showed that women underwent cesarean section in half of the cases (67,6%.).Table 3. Methods of delivery in pregnant women with myocarditis
 |
| |
|
Despite the high rate of abdominal delivery of pregnant women with myocarditis (67.6%), mostly 89% of these women underwent elective cesarean section. Since, pregnant women with myocarditis were registered as a risk group of women of reproductive age. As a consequence, women who are at risk for pregnancy are given general explanatory and enlightening explanations and thorough pregravidarial preparation together with cardiologists at the primary level. Neonatal Apgar score of 8-9 was 86%; 6-7 was 10%; 5 and below was 4% of cases.It is known, that the most common complication of myocarditis during gestation, childbirth, and the postpartum period is the development of circulatory failure (CF). During pregnancy, especially in the second half, there is a physiological increase in circulating blood volume by almost 40-50% [6]. As the degree of CF progresses, this physiological process causes an overload on the heart, with a consequent adverse effect on the condition of the mother and fetus [9]. This in turn contributes to the development and aggravation of obstetric complications. In retrospective analyses, circulatory failure (CF) occurred in 86.3% (176) of women with myocarditis. Of these, CFI - 60.2% (106), CF IIA - 23.7% (54), CF IIB - 9.1% (16) according to a retrospective analysis, there were no patients with CF III, this can be explained by the absolute contraindication to pregnancy in this category of patients. It is especially important to note that in pregnant women with myocarditis, CF developed suddenly during childbirth and after childbirth.
4. Conclusions
Thus, a retrospective analysis showed that myocarditis ranks first among cardiovascular diseases. And among these nosological forms of cardiovascular diseases, the most important, requiring further study, are myocarditis, due to the difficulty of diagnosis, the sudden development of CF during and after childbirth, threatening the life of both the pregnant woman and the fetus.Pregnant women with myocarditis are at risk for the development of circulatory insufficiency and other obstetric and prenatal complications.
References
| [1] | Basman C., Agrawal P.R., McRee C., et al. Diagnostic Approach to Myocarditis Mimicking Myocardial Infarction at Initial Presentation // Cardiol Res. 2016. – Vol. 7(6). – P. 209-213. |
| [2] | Ferreira V.M., Piechnik S.K., Dall’Armellina E., et al. T(1) mapping for the diagnosis of acute myocarditis using CMR: comparison to T2-weighted and late gadolinium enhanced imaging // JACC Cardiovasc Imaging. – 2013. – Vol. 6(10). – P. 1048-1058. |
| [3] | Lassner D, Rohde M, Siegismund Ch, et al. Myocarditis personalized medicine by expanded endomyocardial biopsy diagnostics // World J. Cardiovasc. Dis. – 2014. – Vol. 4(6). – P. 325–340. |
| [4] | Lassner, D., Rohde, M., Siegismund, C.S., et al. Myocarditis personalized medicine by expanded endomyocardial biopsy diagnostics // World J. Cardiovasc. Dis. – 2014. – Vol. 4(6). – P. 325340. |
| [5] | Kobayashi Y, Giles JT, Hirano M, Yokoe I, Nakajima Y, Bathon JM, Lima JA, Kobayashi H. Assessment of myocardial abnormalities in rheumatoid arthritis using a comprehensive cardiac magnetic resonance approach: a pilot study // Arthritis Res Ther. – 2010. – Vol. 12(5). – P. 1-10. |
| [6] | Schaufelberger M. Cardiomyopathy and pregnancy // Heart. – 2019. – Vol. 105. – P. 1543–1551. |
| [7] | Ukena C., Mahfoud F., Kindermann I., et al. Prognostic electrocardiographic parameters in patients with suspected myocarditis // Eur J Heart Fail. – 2011. – Vol. 13(4). P. 398-405. |
| [8] | JCS Joint Working Group. Guidelines for diagnosis and treatment of myocarditis (JCS 2009): digest version // Circ J. 2011. – Vol. 75(3). – P. 734–743. |
| [9] | Cooper L.T. Jr. Myocarditis // N Engl J Med. – 2009. – Vol. 360(15). – P. 1526-1538. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML