-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(3): 630-634
doi:10.5923/j.ajmms.20241403.19
Received: Feb. 12, 2024; Accepted: Mar. 3, 2024; Published: Mar. 6, 2024

Application of Caries Management Program by Assessing Risk Factors in Preschool Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRikhsieva Dilorom1, Tashpulatova Xurshida1, Rakhmatova Sevara2
1Department of Prevention of Dental Diseases of the Tashkent State Dental Institute, Tashkent, Uzbekistan
2Department of Medical and Biological Disciplines in the field of Dentistry of the Kimyo International University in Tashkent, Tashkent, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The prevalence of caries in primary children is over 90% worldwide. Taking these data into account, improving the comprehensive prevention of caries in children will significantly improve dental status and prevent functional disorders of the dentofacial systems. The aim of the research work is to develop modern convenient methods of improving the prevention of caries in children. 40 preschool children between 3-6 years of age were selected as the object of research and their caries indicators were analyzed for 6 months based on the Cambra model. The obtained results show that the number of patients whose caries risk level was initially high, which was 80%, was significantly reduced by 50%, and it is concluded that the program has a positive value in reducing the caries risk level.
Keywords: Caries risk factors, Prevention caries, Children preschool age
Cite this paper: Rikhsieva Dilorom, Tashpulatova Xurshida, Rakhmatova Sevara, Application of Caries Management Program by Assessing Risk Factors in Preschool Children, American Journal of Medicine and Medical Sciences, Vol. 14 No. 3, 2024, pp. 630-634. doi: 10.5923/j.ajmms.20241403.19.
1. Introduction
- According to the classification of the World Health Organization (WHO), dental caries is recognized as a chronic non-communicable disease, which should be paid attention to on a global scale for prevention and treatment measures. The development of dental caries in primary teeth in children may begin early, progress more rapidly in individuals at high risk, and may remain untreated [1]. Negative consequences can affect the quality of life of both the child and their family in the short and long term, as well as cause serious social and economic consequences. Primary teeth perform important chewing, phonetic and cosmetic functions, and also contribute to the normal formation of the jaws and the smooth appearance of permanent teeth. Ignored caries in baby teeth can lead to premature tooth loss before permanent teeth emerge [2,3]. Therefore, it is critical to identify and control primary caries from the time primary teeth emerge to ensure their normal functioning until the permanent teeth emerge. Despite significant improvements in oral health among preschool children in most developed countries over recent decades, dental caries remains a pressing problem affecting a significant proportion of infants and young children [4].Traditional caries treatment methods are symptom-oriented and focus on restorative rehabilitation. However, modern science focuses on treating the causes using caries prevention and minimally invasive dentistry techniques. This is achieved through the implementation of an approach that reduces caries risk factors, increases protective factors against caries and manages the caries process through risk assessment using the CAMBRA program (Caries Management By Risk Assessment) caries management based on risk assessment. Caries risk assessment (CRA - Caries Risk Assessment) is an important component of an individually focused approach. The American Academy of Pediatric Dentistry (AAPD) recognizes that the use of caries risk assessment protocols and appropriate treatments can greatly facilitate clinician decision-making. [5,6,7]. In the CAMBRA (Caries Management by Risk Assessment) approach, disease indicators are clinical signs of past caries activity, such as the presence of carious lesions or restorations. CAMBRA places particular emphasis on determining each patient's caries risk level, which represents the first step in managing the disease process. This is achieved by identifying specific clinical indicators of the disease, risk factors and protective factors for each individual [8]. A caries management model is then implemented that incorporates various factors such as diet, fluoride exposure, body susceptibility and oral microflora composition. This model also takes into account the interaction of social, cultural and behavioral factors, making it more widely applicable and personalized [9,10]. Assessing the level of risk for future dental caries is an important first step in caries management and in monitoring oral health over time. Effective management of early childhood caries requires a risk-based approach to develop an individualized treatment plan.
2. Materials and Methods
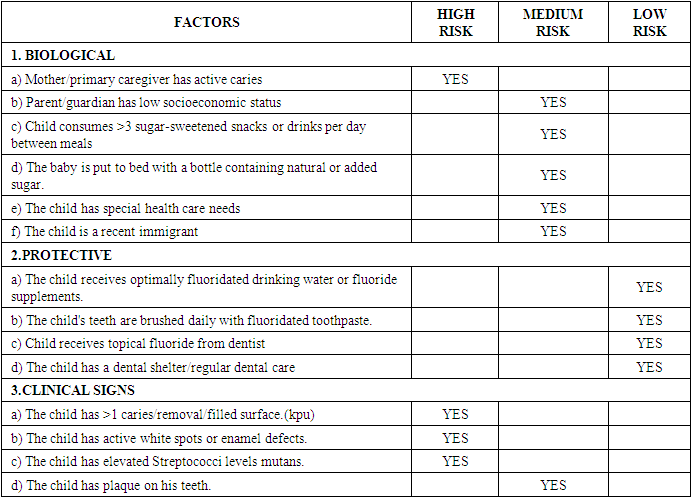
- 40 preschool children aged 3-6 years, as well as their guardian parents, were randomly selected as the object of the study in order to obtain complete information about the object of the study. The methods used were clinical examination, bacteriological testing, and answering questions. All children were examined and assessed using the CAMBRA protocol (a dental caries risk assessment form recommended by the American Academy of Pediatric Dentistry). Academy of Pediatric Dentistry, 2016). It is divided into four columns. The first column lists three risk factors: biological, protective, and clinical. The second, third and fourth columns indicate the risk classification (high, medium and low risk) (Table 1). Data were collected in public kindergartens and a simplified form was used. The caries risk assessment form for children aged 0 to 6 years consisted of 5 biological factors, 4 protective factors and 3 clinical data. A child's risk rating (low, moderate, or high) is determined by describing the conditions that apply to the individual patient and the factors that promote or protect against dental caries. Initial data were collected through questionnaires provided by parents or guardians. Risk factors were analyzed according to the Kerry scale (Table 2), which served as the basis for the implementation of appropriate preventive measures and treatment methods. The risk assessment scale includes 12 factors, including biological factors and clinical signs, as well as protective elements. For each factor, participants were assigned a score based on their risk or protective effect. This system was likely designed to create individual risk scores for each participant. For example:- If there was a high-risk biological or clinical factor, the participant received +2 points.- If there was a medium risk factor, the participant received +1 point.- In protective factors, when they were absent, the participant received -1 point.
|
|

3. Results
- Of the 40 participants, 18 were boys (45%), 22 were girls (55%), and ranged in age from 3 to 6 years. 12 factors were considered to classify the risk of caries lesions and formed a scale to determine caries risk assessment factors. Children selected for the study were screened for CAMBRA factors. Information was collected through questionnaires from their parents or close guardians. The initial data collection was analyzed, risk factors were calculated and divided into levels according to the Kerry scale, and the necessary preventive measures and treatment methods were introduced. The results were rechecked and analyzed dynamically after 1, 3, 6 months (Table 3). Our results showed that when applying the CAMBRA protocol, according to the analysis of the results, the number of children with low risk was initially 3 (7.5%), but after 6 months this number increased to 10 (25%), respectively, the number of children at high risk decreased from 32(80%) at baseline to 20(50%) after 6 months.
|

4. Discussion
- The protocol is tailored based on the level of risk, including the use of fluorotherapy, gel and varnish, making behavioral changes (advice on diet and frequency of brushing), providing minimally invasive care (application of sealants), and ensuring the adequacy of the parent's oral environment. Effective caries risk assessment helps identify those in need of preventive services and helps manage risk factors. The results highlight the importance of individualized care pathways for children in the context of caries treatment and prevention. Individualized decisions based on risk level, age, and adherence to preventive strategies provide a higher chance of success, reduce the likelihood of complications, and provide a more efficient use of resources than a standardized treatment approach. There are medical, social, and economic effectiveness of improving measures to prevent caries in children based on the above-mentioned program:Medical efficiency are:• Early risk identification: The use of the CAMBRA protocol allows for early assessment of caries risk, which allows dentists and healthcare professionals to identify risk factors in the early stages and take measures to control them.• Individualized approach: Assessment of caries risk, taking into account biological, clinical and protective factors, allows the development of individualized treatment and prevention plans. This approach allows for more accurate prediction and management of oral health for each patient.• Efficient use of resources: By identifying individual risk and protective factors, medical resources can be more effectively directed toward higher-risk patients requiring more intensive interventions.Social efficiency are:• Improving children's lifestyle and health: Proactive use of the protocol allows risk factors to be identified and lifestyle interventions taken, such as dietary changes, reducing sugar intake and improving oral care. This affects children's health by reducing the risk of dental caries and improving their quality of life.• Strengthening social interaction: The process of involving parents/guardians in the risk assessment and treatment plan creates interaction between patients and health care personnel. This can help strengthen social connections and promote positive attitudes toward health care.• Improving health literacy among parents and caregivers: The CAMBRA protocol includes interaction with parents and caregivers, providing recommendations for child oral care. This promotes health literacy among parents and caregivers, which can lead to healthier lifestyles for children.Economic efficiency are:• Reduced treatment costs: Proactive risk assessment and early intervention can prevent the development of caries and related complications. This reduces the cost of expensive dental treatment and restoration, and also reduces the need for emergency medical care.• Optimizing the use of health care resources: Individual strategies based on risk assessment allow for more efficient use of health care resources. Providing more precise and targeted prevention and treatment interventions aims to improve outcomes and reduce costs.• Reduced need for complex surgical restorations: Early identification and management of caries risk reduces the likelihood of developing complex forms of caries that require expensive surgical restorations. This saves money that could have been spent on more intensive treatment measures.
5. Conclusions
- n Based on data from the CAMBRA protocol, we conclude that early caries risk assessment is fundamental to the prevention and effective management of caries in children 0 to 6 years of age. This approach allows children at high risk to be identified and proactive measures to be taken to prevent the development of the disease.n The CAMBRA protocol, which includes assessment of biological, clinical and protective factors, provides a comprehensive approach to risk management. Individualized strategies developed based on these data appear to be more successful in reducing the incidence of dental caries in children.n The CAMBRA protocol and individualized risk management strategies make economic sense. Reducing treatment costs, optimizing the use of resources and preventing costly complications contributes to more efficient use of funds in the healthcare system.This includes regular visits, assessing the effectiveness of prevention measures and adjusting strategies if necessary. Advantages of CAMBRA include its adaptability, rapid application, and effectiveness in developing individualized treatment plans. The protocol promotes earlier identification of caries risk and provides tools for making more informed decisions regarding preventive and treatment interventions. It should be noted that standardized protocols such as CAMBRA play an important role in dental health management and caries prevention in children, ensuring more efficient use of resources and improving the quality of life of children.