-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(3): 616-619
doi:10.5923/j.ajmms.20241403.16
Received: Feb. 3, 2024; Accepted: Feb. 23, 2024; Published: Mar. 6, 2024

Assessment of Risk Factors Affecting the Development of Chronic Kidney Disease in Women of Fertile Age
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMakhmudov R. B., Akhmedova N. Sh.
Bukhara State Medical Institute named after Abu Ali I bn Sina, Bukhara, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

In recent years, the world community has been faced with a global problem that has not only medical, but also enormous socio-economic significance - a pandemic of chronic diseases that annually claim millions of lives, lead to severe complications associated with loss of ability to work and the need for highly costly treatment. The purpose of the study is to assess risk factors for the development and progress of chronic kidney disease. Materials and methods. 281 women were examined living in the territory of the Bukhara district and Gijduvan district of the Bukhara region. A screening questionnaire has also been tested to assess factors influencing the development of chronic kidney disease. Results: Based on the results of the examination, the most significant risk factors for chronic kidney disease were identified. The use of prognostic criteria makes it possible to improve the quality of examination and form risk groups at the primary health care level.
Keywords: Chronic kidney disease, Fertile age, Glomerular filtration rate
Cite this paper: Makhmudov R. B., Akhmedova N. Sh., Assessment of Risk Factors Affecting the Development of Chronic Kidney Disease in Women of Fertile Age, American Journal of Medicine and Medical Sciences, Vol. 14 No. 3, 2024, pp. 616-619. doi: 10.5923/j.ajmms.20241403.16.
1. Introduction
- Currently, the problem of chronic kidney disease in the world is global in nature and is characterized by high prevalence, a steadily increasing incidence of complications, and also causes significant economic damage [4].Kidney pathology occupies an important place among chronic non-infectious diseases due to its significant prevalence, sharp decline in quality of life, high mortality and leads to the need for expensive methods of replacement therapy in the terminal stage - dialysis and kidney transplantation.The prevalence of CKD is comparable to such socially significant diseases as hypertension and diabetes mellitus, as well as obesity and metabolic syndrome. Signs of kidney damage and/or decreased glomerular filtration rate are detected in at least every tenth representative of the general population. Moreover, comparable figures were obtained both in industrial countries with a high standard of living and in developing countries with middle and low income [4,6].The problem of screening for chronic kidney disease is very serious. Its solution is only possible with close cooperation between doctors of different specialties. On the other hand, it is necessary integration of nephrology and primary care, as well as other specialties, in order to carry out broad preventive measures, early diagnosis of CKD, ensure continuity of treatment and effective use of available resources. There are several ways to identify CKD, including the determination of CKD markers in patients undergoing examination for various diseases. One important way to identify CKD is through conditional testing. - healthy population in which there are risk factors for the development of CKD.The purpose of this study is identification of risk factors for CKD by surveying the rural population and assessing the importance of risk factors for the development and progress of CKD.
2. Materials and Methods
- The study included 281 women living in the territory of family clinic No. 2 (Dekhozhi) of Bukhara district and family clinic Zarangari Gijduvan district, Bukhara region.All subjects underwent a survey, which included questions regarding age, place of work, the presence of concomitant diseases and conditions, adherence to a healthy lifestyle, anthropometric data, height, weight; body mass index (BMI) was calculated using the Ketle formula, depending on which was distinguished as normal body weight - with BMI<25, overweight BMI=25-30, obesity BMI>30. Blood pressure was measured. They found out the presence in the present or past of diabetes mellitus or episodes of increased sugar, cholesterol, changes in urine tests, arterial hypertension, nephropathy in pregnant women and kidney disease in direct relatives, abuse of analgesics and non-steroidal anti-inflammatory drugs. “craving” for salty and bitter foods, the presence of chronic infections such as tonsillitis, dental caries and bad habits.All subjects underwent urine analysis using Combina 13 test strips (Human GmbH Germany). These diagnostic test strips are designed to provide a semi-quantitative measurement of microalbumin concentration in urine. The test for measuring MAU in urine is based on the principle that the color of the indicator changes under the influence of proteins. The level of MAU was determined according to the following scale: up to 10 mg/l normal, 10-30 mg/l initial increase, 30-80 mg/l average increase, 80-150 mg/l high level [3,6,9]. In order to interpret the data obtained, a methodological approach was used by a number of researchers who used it to assess various factors (Monakhov B.P. 1984; Nasreddinov H.K. 1995; Atamuradov Sh.I. 1996, etc.).For In the integral assessment of factors and their gradations, it is imperative to select a standard value (M), based on which the standardization intensive indicators (NIP) were calculated. The relative risk indicator RR or RR was determined (from the English " relative "risk"). In this case, the analysis involved 9 groups of factors, the role of which in the occurrence and development of CKD has been shown by numerous researchers. In particular, age, all, bad habits, drug abuse, hypertension, coronary artery disease, diabetes mellitus and primary kidney pathology in patients and direct relatives, history of nephropathy and proteinuria in women and UIA.Relative risk is the most important indicator in prescribing certain treatments or conducting studies with possible side effects.The relative risk value is determined by the following formula:
 where A, B, C, D – the number of observations in the cells of the contingency table.This method allows you to analyze four -field tables.
where A, B, C, D – the number of observations in the cells of the contingency table.This method allows you to analyze four -field tables.3. Results and Discussion
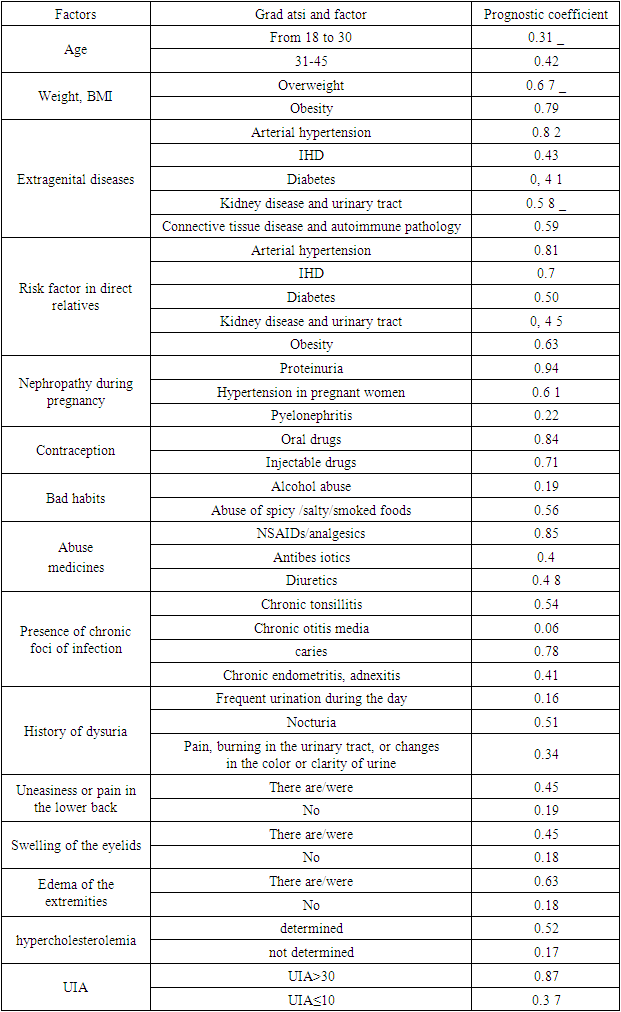
- The prevalence of CKD was assessed by the level of MAU>30 mg/l and the glomerular filtration rate (GFR), after which the patients were divided into 2 groups.The first group consisted of 119 patients with CKD (MAU>30 mg/l, GFR <90 ml/min, 1.73 m2) aged 18-25 years (average age 37.9±6.1 years).The second group is a risk group for the development of CKD (MAU>30mg/l, GFR>90ml/min, 1.73m2). This group consisted of 161 students, average age 32.7 ± 3.5 years.Based on the results of the questionnaire, our data confirms that old age is one of the leading risk factors for the development of CKD (44%) than in young and middle-aged people - 23 and 34% (p <0.001).The role of arterial hypertension and coronary artery disease as one of the most important risk factors for the development and progression of CKD is well known. In our studies, the frequency of detection of this factor was 34% and 18.3%. The most sensitive predictors were a history of proteinuria and abuse of analgesics and NSAIDs, with detection rates of 44.8% and 34.2%.To assess the value of risk factors, the “relative risk” indicator was calculated, which is defined as the ratio of the maximum and minimum values of degrees atsi th of each factor. By relating these two values, one can obtain the relative risk coefficient for a given factor. At the next stage, the integral value (NIP * OR factor) is calculated. After appropriate calculation of scores for all factors, the maximum and minimum values in degrees of each factor were determined (Table 1).
|
|
4. Conclusions
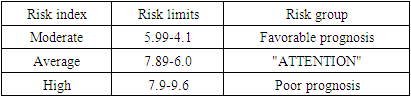
- Taking into account the developed risk factors, 281 women suspected of having CKD were examined and the risk limits were determined. At the same time, patients with a moderate risk of the index amounted to 38.8% (n = 109), a medium risk group with a prognosis of “ATTENTION” 46.6% (n = 131) and a high risk group with an “unfavorable prognosis” 14.6% (n =41).The most numerous was the group of subjects with an average risk index a, with such risk factors for the development of CKD as the use of contraception, arterial hypertension, coronary artery disease in patients and in direct relatives, increased BMI, diabetes mellitus, bad habits, mainly the consumption of a lot of salt and the abuse of NSAIDs.Taking into account the position of screening the population to identify CKD, as well as the high cost and labor intensity of laboratory tests when conducting mass examinations in population groups, it is proposed to conduct a questionnaire to identify prognostically significant risk factors with the subsequent calculation of a risk index for the development of CKD. According to the results of the study, based on the criteria for diagnosing CKD, with detection of chronic kidney disease, further examination and treatment is recommended.