-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(3): 597-601
doi:10.5923/j.ajmms.20241403.12
Received: Feb. 6, 2024; Accepted: Feb. 27, 2024; Published: Mar. 6, 2024

Clinical and Radiological Manifestations of Partial Intestinal Obstruction in Newborns and Infants
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSattarov Zh. B., Ibragimov A. V.
Tashkent Pediatric Medical Institute, Republican Training, Treatment and Methodological Center for Neonatal Surgery at the Republican Perinatal Center, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article presents data on examination of 123 patients with congenital intestinal obstruction out of 463 children with various forms of congenital intestinal obstruction. Their clinical presentation in upper and lower partial intestinal obstruction is presented. The results of radiological methods, indications and the sequence of application of simple radiography, irrigography and passing through the gastrointestinal tract are presented.
Keywords: Congenital partial intestinal obstruction, Clinical presentation, Anatomical forms, Diagnosis, Newborns, Children of weaning age
Cite this paper: Sattarov Zh. B., Ibragimov A. V., Clinical and Radiological Manifestations of Partial Intestinal Obstruction in Newborns and Infants, American Journal of Medicine and Medical Sciences, Vol. 14 No. 3, 2024, pp. 597-601. doi: 10.5923/j.ajmms.20241403.12.
1. Relevance
- Despite the increasing incidence of intestinal obstruction in children [5], there are only a few publications in the literature devoted to this problem. Some authors mention the membranous form of atresia, although in most of the described cases there was a complete membrane of the colon, identified intraoperatively during the neonatal period [2,5].The incidence of congenital intestinal obstruction (CIO) is 1:1500-1:2000 newborns. Various forms of CIO in most cases occur in the neonatal period and up to 3 months of age [1,4,9,12]. There are known examples of manifestations of intestinal obstruction in children of older age groups, adolescents and even adults. There is no detailed analysis in the literature of the frequency, forms and results of treatment of older children and adults with this pathology. A few works highlight methods of diagnosis and surgical treatment in individual cases [3,4,6,11].There are subacute, chronic and recurrent forms of CIO. With obstructions that cause partial obstruction of patency from the inside of the intestine (stenosis, membranes with lumen, doubling of the gastrointestinal tract) or compression of the intestine from the outside, caused by malformations and tumors of other organs, abnormal arrangement of the vessels of the abdominal cavity, unusual structure and fixation of ligaments and other formations of the peritoneum, gradual progression of clinical signs of gastrointestinal obstruction in the form of chronic intestinal obstruction [4,7,12].The clinical picture, characteristic of almost all types of intestinal obstruction, consists mainly of such symptoms as: abdominal pain, nausea, vomiting, lack of stool, and the passage of gas. With the development of complications, peritoneal symptoms of systemic disorders appear. The course of the disease depends on the etiological factor and characteristics of pathogenesis. Among the methods of radiation diagnostics, the most informative are ultrasound and x-ray examination. Especially ultrasound of the abdominal cavity, the reliability of which reaches 96%. X-ray examination, as a traditional method of examining intestinal obstruction, is available in all medical institutions [1,4,7,8].There are many controversial issues in the diagnosis and treatment of children with CIO that require a unanimous decision.The purpose of this study is to study the features of the clinical course and radiological manifestations of partial intestinal obstruction in newborns and infants.
2. Materials and Methods
- In the Republican Training, Treatment and Methodology Center for Neonatal Surgery at the Russian Orthodox Church, at the clinical base of the Department of Hospital Pediatric Surgery of the Tashkent Pediatric Medical Institute, in 2015-2022, 463 children with various surgical diseases of the abdominal organs, manifested by congenital intestinal obstruction, were treated. Of 123 (26.6%) newborns and infants with various forms of CIO, 99 (80.5%) newborns were aged from 1 day to 1 year; up to 3 months – 19 (15.5%); up to 7 months – 3 (2.4%); up to 1 year – 2 (1.6%). In 105 (85.4%) patients, high partial intestinal obstruction was established, in 18 (14.6%) – low. of 64 (52.0%) children with defects of intestinal rotation and fixation, intestinal obstruction was: high - in 31 (93.75%), low - in 24 (6.25%). Among the patients, boys predominated - 51 (41.5%), girls were 72 (58.5%). The patients underwent complex clinical, laboratory and radiation diagnostic methods (ultrasound, radiological - plain radiography of the abdominal organs, contrast study of the gastrointestinal tract, irrigography and CT), aimed at an objective assessment of the somatic status, the course of transient conditions and determining the form of CIO, the nature of the accompanying developmental anomalies and somatic diseases affecting the course and outcome of the disease.
3. Research Results
- Based on the results of treatment of 123 children with CIO of various forms, localization and causes of obstruction in accordance with the generally accepted classification, we determined the frequency of individual nosological forms, systematized their clinical manifestations, features of the course, summarized the results of auxiliary research methods, and identified the nature of associated anomalies. These data are of fundamental importance due to the fact that, with individual differences in clinical and radiological manifestations and complications characteristic only of high or low intestinal obstruction, the same clinical and radiological picture is observed, regardless of the cause of obstruction in the corresponding localization.With high intestinal obstruction, partial obstruction was caused by duodenal stenosis - in 6 (3.9%) patients; compression of the duodenum by the annular pancreas – in 10 (3.9%); external compression of the organ by periduodenal adhesions - in 11 (2.3%); the presence of a membrane with a lumen – in 18 (14.7%). In 60 (48.1%) cases, duodenal obstruction was caused by various forms of intestinal malrotation. 1 of 23 patients with low intestinal obstruction, in 18 (69.2%) the phenomena of partial obstruction predominated. Membranes with lumen were noted in 4 (1.2%) patients; stenoses – in 3 (2.0%). Compression of the small intestine by adhesions and pathological formations in 7 (9.1%) patients caused partial intestinal obstruction. Various forms of intestinal malrotation in 4 (30.8%) children were accompanied by clinical and radiological signs of low intestinal obstruction.With intestinal CIO, various combined anomalies of the gastrointestinal tract and other organs and systems are observed. In 76.4% of patients, CIO manifested as an isolated pathology; in 23.6% it was combined with other forms of CIO.In acute intestinal obstruction, including CIO, an informative diagnostic method is x-ray examination. The feasibility of using this method separately or in combination is determined individually. The examination begins with a survey X-ray of the abdominal cavity (in newborns, covering the chest) with the child in an upright position.The most common findings are two gas bubbles with a horizontal liquid level. This corresponds to a distended stomach and duodenum and indicates obstruction of the distal duodenum.Multiple levels are characteristic of low intestinal obstruction. A distended stomach without intestinal pneumatization indicates volvulus (Fig. 1).
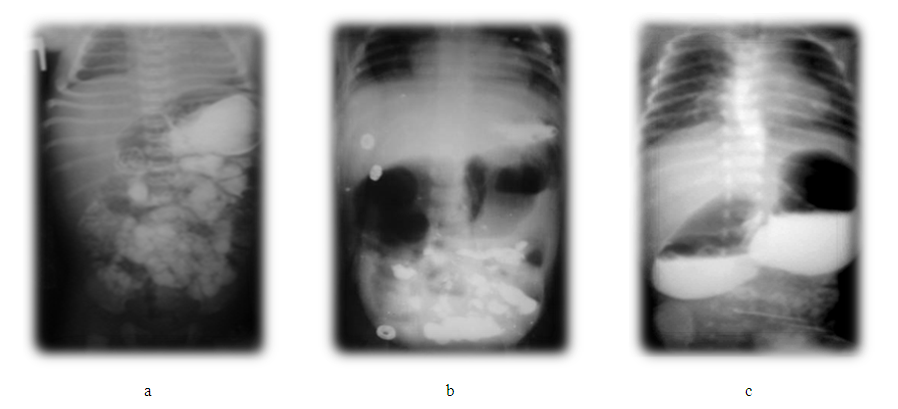
 | Figure 1. Plain radiography for intestinal obstruction: a) the presence of two fluid levels with high intestinal obstruction; b) accumulation of gas in the dilated colon with low intestinal obstruction; c) the “silent” zone and the initial parts of the small intestine filled with gas indicate malrotation of the midgut |
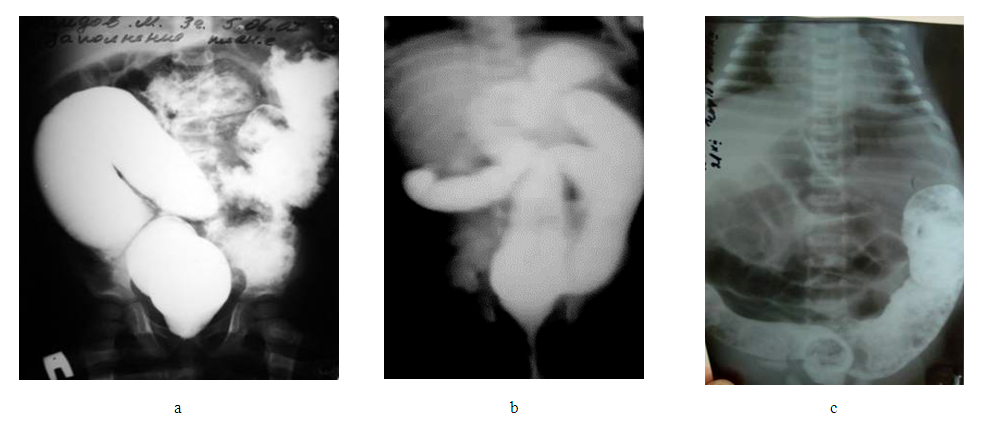 | Figure 2. Contrast irrigograms: a) tight filling of the distal colon, partial passage of contrast into the overlying sections at the membrane of the sigmoid colon; b) high location of the cecum with intestinal malrotation; c) delay of contrast in the sigmoid colon with stenosis of the colon |
 | Figure 3. Passage of contrast through the gastrointestinal tract: a) partial high intestinal obstruction; b) partial low intestinal obstruction; c) changes in the size, shape and syntopy of the duodenum |
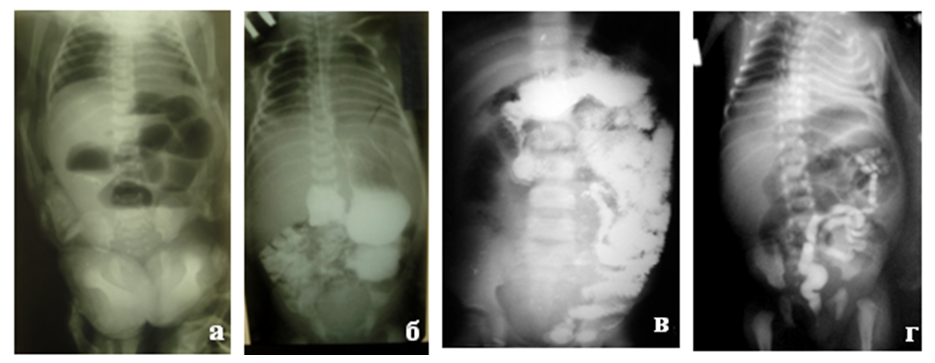 | Figure 4. Radiographs of a mesocolcoparietal hernia: a) plain radiography - uneven pneumatization of small intestinal loops with signs of low intestinal obstruction; b-c): passage of contrast through the gastrointestinal tract in right-sided localization (b); with left-sided localization (c) – contrasted parts of the small intestine are localized mainly on the right and left; d) irrigogram – identifies an incorrectly located colon in the form of microcolons |
4. Conclusions
- The clinical picture of CIO in newborns and infants is dominated by signs of high or low partial intestinal obstruction, depending on the degree of obstruction, the nature of the complications encountered and concomitant pathology. Clinical signs of intestinal perforation, peritonitis with symptoms of intestinal obstruction and volvulus should be considered a risk of complications of intestinal malrotation.Analysis of our material shows that the phenomena of recurrent intestinal obstruction, retardation of the child in physical development, paroxysmal abdominal pain, chronic constipation should cause doctors to be increasingly wary of CIO. Suspicion of such anomalies is justified in the following radiological signs: distended gas bubble of the stomach; phenomena of partial intestinal obstruction; atypical arrangement of loops of the small and large intestines; lengthening of the colon.Data from preoperative X-ray studies are the most informative, but do not always allow us to identify the anatomical form of CIO. With an integrated approach to diagnosis, its accuracy increases. The final diagnosis is verified during surgery.