Malikova Gulsanam1, Abdurakhmanov Bakhtiyor2, Kodirov Javlon3
1Head of the Gynecology Department of the Multi-Network Clinic of the Center for the Development of Professional Qualifications of Medical Workers, Okhangaron District, Tashkent Region, Uzbekistan
2Researcher, 2nd Department of Obstetrics and Gynecology, Center for the Development of Professional Qualifications of Medical Workers, Okhangaron District, Tashkent Region, Uzbekistan
3Head of the Okhangaron Medical Association of the Tashkent Region, Okhangaron District, Tashkent Region, Uzbekistan
Correspondence to: Malikova Gulsanam, Head of the Gynecology Department of the Multi-Network Clinic of the Center for the Development of Professional Qualifications of Medical Workers, Okhangaron District, Tashkent Region, Uzbekistan.
| Email: |  |
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Prevention of postoperative adhesions is the main problem of surgical treatment of infertility in women, which cannot be solved even with the use of microsurgical techniques, which, although it reduces the formation of adhesions, does not completely exclude this possibility. Results of restoration of reproductive function in women after surgery and rehabilitation can vary depending on the individual's specific condition and response to treatment. However, successful outcomes may include improved fertility, increased chances of natural conception, or better outcomes from assisted reproductive technologies such as in vitro fertilization (IVF). It's important for women undergoing surgical treatment for intracanalicular infertility to work closely with their healthcare team to ensure comprehensive care before, during, and after the procedure.
Keywords:
Intracanalicular infertility, Fallopian tube, Restoration of patency, Pregnancy
Cite this paper: Malikova Gulsanam, Abdurakhmanov Bakhtiyor, Kodirov Javlon, Tactics of Surgical Treatment of Women with Intracanalicular Infertility and Results of Restoration of Reproductive Function in Women after Surgery and Rehabilitation in the Postoperative Period, American Journal of Medicine and Medical Sciences, Vol. 14 No. 2, 2024, pp. 527-531. doi: 10.5923/j.ajmms.20241402.74.
1. Introduction
Infertility, that is, the inability to have offspring, is a serious condition that disrupts a person’s social and psychological adaptation, affecting his health and quality of life. Because of this, infertility in the family remains one of the most important medical and government problems. According to world statistics, every 5 married couples suffer from infertility, and therefore this problem remains relevant [1,2]. Numerous studies carried out in the CIS and abroad have been devoted to the study of this problem [3,4,5,6,7,8]. The frequency of infertile marriage, according to a number of authors, ranges from 10-15% to 18-20%. The cause of an infertile marriage in 40-50% of cases is a pathology of the reproductive system in one of the spouses, less often (5-10% of cases) in both. In 60-80% of such marriages, the cause of infertility is the woman’s health, and in 30-40% it is the husband’s illness.Timely treatment of extragenital diseases, improvement of social, everyday and family relationships often force women to restore their generative function. Infertility of endocrine origin can be treated with medication, and peritoneal forms of infertility can be successfully treated by endoscopic salpingolysis, i.e. Treatment of infertility of intracanalicular origin requires its own methodological approach. The effectiveness of surgical treatment of tubal infertility largely depends on the correct management of patients after surgery.Prevention of postoperative adhesions is the main problem of surgical treatment of infertility in women, which cannot be solved even with the use of microsurgical techniques, which, although it reduces the formation of adhesions, does not completely eliminate this possibility. Adhesions after surgery occur as a result of infection and tissue trauma, the development of endometriosis and other various factors [9,10].
2. Purpose of the Research
In order to restore the generative function of 90 women with intracanalicular infertility, restore the patency of the fallopian canal using an innovative technique.
3. Materials and Methods
90 women suffering from tubal intracanalicular infertility at the age of 24–30 years were subjected to surgical treatment. Analysis of the genesis of occlusion and stenosis in the examined patients showed that 69 women (60.2%) had a history of surgical interference - appendectomy, ectopic pregnancy, ovarian apoplexy, ovarian resection, etc. the remaining 29 women had a history of chronic salpingo-oophoritis. In all examined patients, hysterosalpingography and therapeutic hydrotubation revealed obstruction of the intracanalicular canal of the fallopian tube.
4. Results and Discussion
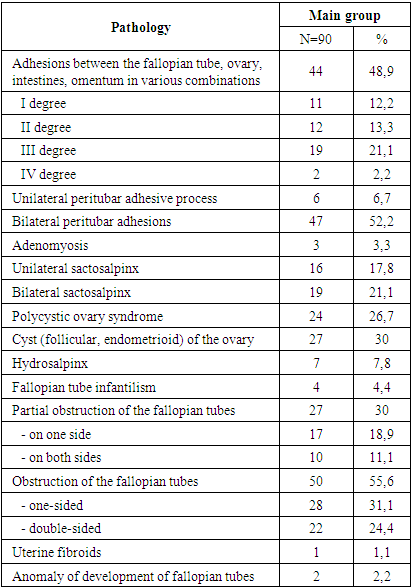
As a result of diagnostic measures, data obtained on the causes of infertility and the condition of the uterus, fallopian tubes and ovaries, the treatment tactics for patients with intracanalicular infertility were determined. At the same time, surgical treatment was carried out aimed at eliminating adhesions in the pelvis, removing endometrioid heterotopias, removing ovarian cysts, decortication of ovarian tissue, conservative myomectomy and reconstructive operations on the fallopian tubes. The laparotomy picture of the pathological process in intracanalicular infertility is presented in Table 1.Table 1. Pathological processes detected during laparotomy
 |
| |
|
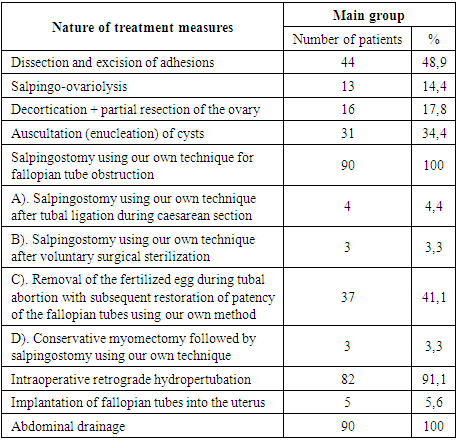
When examining the pelvic organs and abdominal cavity, the most common was the adhesive process between the fallopian tube, ovary, intestines and omentum in various combinations, which occurred in 44 patients of the main group. Thus, grade 1 adhesion were detected in 11 patients of the main group; 2nd degree – in 12 patients of the main group; 3rd degree - in 19 patients of the main group and 4th degree - in 2 women of the main group we examined. Adhesions between the uterus, uterosacral ligament, right and left appendages, and intestines were found in 21 women of the main group, which is 23.3%. Adhesions between the uterus, uterosacral ligaments and appendages occurred in 9 (10%) patients of the main group. Between the uterus, uterosacral ligaments, appendages and bladder, adhesions were found in 3 (3.3%) women of the main group. Adhesions between the omentum and the anterior abdominal wall – in 9 (10%) women of the main group. The adhesive process of the retrouterine space was observed in 3 (3.75%) women of the main group. Peritubar adhesions were detected in 53 (58.9%), and unilateral peritubar adhesions were detected in 6 (6.7%) and bilateral peritubar adhesions in 47 (52.2%) patients of the main group. Sactosalpinx occurred in 35 patients (38.9%), with unilateral sactosalpinx in 16 (17.8%) and bilateral sactosalpinx detected in 19 (21.1%) women of the main group. It should be noted that hydrosalpinx was found in 7 (7.8%) women of the main group. Adenomyosis occurred in 3 (3.3%) women in the main group. The combination of polycystic ovaries with adhesions occurred in 24 (26.7%) women of the main group. Ovarian cysts, including follicular and endometrioid cysts, were found in 27 (30%) patients of the main group. Partial obstruction of the fallopian tubes in 27 (30%), and unilateral in 17 (18.9%) and bilateral in 10 (11.1%) women was identified in the main group, including of which infantilism of the fallopian tubes was detected in 4 (4.4%) women. Fallopian tube obstruction occurred in 50 (55.6%) women in the main group, unilateral in 28 (31.1%) and bilateral in 22 (24.4%) women in the main group. An anomaly in the development of the fallopian tubes was detected in 2 (2.2%) patients of the main group. Thus, among all the pathologies in women with intracanalicular infertility, adhesions in the pelvis and abdominal cavity, polycystic ovaries, ovarian cysts and their combinations predominate. This requires an individual approach to the treatment of each woman and the development of appropriate rehabilitation measures. Depending on the nature of the detected pathology, appropriate surgical interventions were performed, the type and extent of which are presented in Table 2.Table 2. Scope of operations for intracanalicular infertility N=90
 |
| |
|
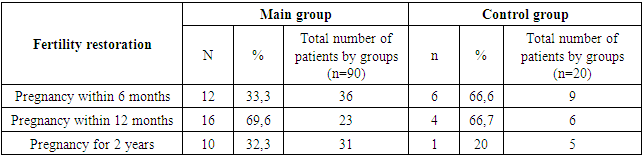
When analyzing the surgical operations performed by us on the women we examined, in 44 (48.9%) patients of the main group, dissection and excision of adhesions were performed during surgery. Salpingo-ovariolysis was performed in 13 (14.4%) patients of the main group with peritubar and periovarial adhesions as an intraoperative stage, necessarily preceding the stage of tubal plastic surgery and intervention on the ovaries for the purpose of surgical correction of their disorders. Salpingo and ovariolysis always began with the mobilization of the fallopian tubes and ended with the restoration of mobility and normal topographic location of the ovary. It should be noted that 24 (26.7%) women in the main group had vesicular rashes on the surface of the uterus, which probably indicates an exacerbation of the inflammatory process of viral etiology. The membrane of the ovaries was yellowish-white to grayish. In 24 (26.7%) cases, a dense tunica albuginea (polycystic ovary syndrome) was determined. Under the tunica albuginea, old corpora lutea were visualized, and in their place were scars and follicles at various stages of development. In 31 (34.4%) women of the main group, ovarian cysts were enucleated. For endometrioid heterotopias of the ovary, decortication was performed by partial resection of the ovary in 16 (17.8%) cases. Conservative myomectomy was performed in 3 (3.3%) women in the main group. In case of ectopic pregnancy, including tubal abortion, the fetal egg was removed with subsequent restoration of the patency of the fallopian tubes using our own method in 37 (41.1%) cases. Salpingostomy was performed using our own technique for fallopian tube obstruction in 90 (100%) women of the main group. In the genesis of fallopian tube obstruction, the inflammatory reaction was quite often caused by chronic chlamydial, mycoplasma, viral infection, confirmed by enzyme immunoassay and immunofluorescent analysis. The physiological functions of the fallopian tubes were restored in 4 (4.4%) cases after tubal ligation during cesarean section; In 3 (3.3%) women of the main group, salpingostomy was performed using their own technique after voluntary surgical sterilization. 5 (5.6%) women of the main group indicated amputation of one fallopian tube due to tubal pregnancy or ovarian cysts; they underwent implantation of the fallopian tubes into the uterus, followed by salpingostomy using their own technique on both sides. Retrograde hydropertubation was performed intraoperatively in 82 (91.1%) cases. Drainage of the abdominal cavity was performed in 90 (100%) in order to prevent pelvic adhesions for the gradual introduction of rheopolyglucin up to 20.0 ml 2 times a day. A dioxedine solution of 10 ml was administered intraoperatively to prevent the development of secondary purulent-septic complications and adhesions. The following was administered intravenously during the operation: for the purpose of preventing purulent-septic complications in the postoperative period - rovamycin 1.5 million units. in 100 ml - 0.9% sodium chloride; claforan 1.0 at 0.9% -10.0 ml saline. solution, for patients with torch infections of viral etiology, Zovirax 250 mg in 200 ml - 0.9% sodium chloride. The remaining patients, depending on sensitivity to antibiotics, were administered parenterally according to the generally accepted regimen. No postoperative complications were observed in postoperative patients. Wound healing Per I (100%).The results of rehabilitation therapy for women with intracanalicular infertility are shown in Table 3. Table 3. Restoring fertility in women after recanalization of the fallopian tubes using an innovative technique
 |
| |
|
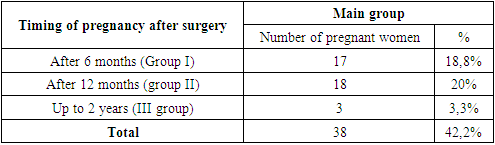
Analysis of the results of restoration of fertility in women with intracanalicular infertility shows the following: among patients, pregnancy occurred within 6 months in 33.3% in the main group and in 66.6% in the control group; among patients pregnant within 12 months, this figure was 69.6% and 66.7%, respectively; pregnancy within 2 years was 32.3% in the main group and 20% in the control group.The duration of the period from the moment of surgical correction and subsequent drug treatment until pregnancy in women with intracanalicular infertility is described in Table 4.Table 4. Timing of pregnancy after restoration of patency of the fallopian tubes. N=90
 |
| |
|
According to the table, during the first 6 months after the operation, pregnancy occurred in 17 women in the main group, which amounted to 18.8%. Within 6-12 months after the operation, pregnancy occurred in 17 (18.8%) women in the main group. From 16 months to 2 years after surgery, pregnancy occurred in 3 (3.3%) women in the group. The total pregnancy rate after comprehensive pre- and postoperative rehabilitation treatment was 42.2% in the main group. The outcome of pregnancy in women with restored generative function after infertility of intracanalicular origin is presented in Table 5. Table 5. Pregnancy outcome in women with restored generative function after infertility of intracanalicular origin in the main group
 |
| |
|
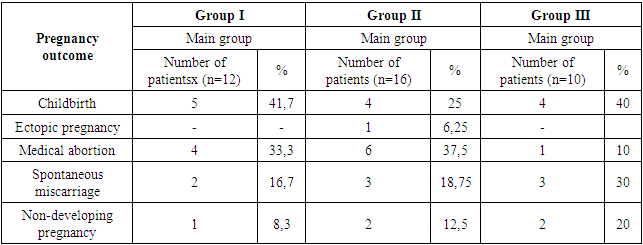
Pregnancies ended in childbirth: within 6 months (in group I) in 41.7% of women in the main group; within 16 months (in group II) in 25% of women in the main group; for 2 years (in group III) in 40% of women in the main group. Medical abortion (MA) due to severe vomiting syndrome ended in 4 (33.3%) pregnancies in the group; for social reasons, 6 (37.5%) pregnancies in group II ended, 1 (10%) pregnancies in group III. In group II, ectopic pregnancy (EP) occurred after surgery in the 7th month in 1 (6.25%) women in the main group. Spontaneous miscarriage (SPM) in the first trimester of pregnancy occurred in 2 (16.7%) MG patients in group I, 3 (18.75%) MG women in group II and 3 (30%) MG women in group III. Non-developing pregnancy (NP) occurred in 1 (8.3%) OG patients in group I, 2 (12.5%) OG women in group II and 2 (20%) OG women in group III. The outcome of pregnancy in 1 (8.3%) women from the OG (group I) and 1 (6.25%) women from the MG (group II) is unknown due to a change in their permanent place of residence.
5. Conclusions
1. Surgical treatment for patients with intracanalicular infertility should be carried out after a complete clinical examination and restoration of the hypothalamic-pituitary, ovarian and uterine menstrual cycles.2. In case of intracanalicular infertility, it is necessary to surgically restore the patency of the fallopian tube in somatically healthy women of reproductive age using an innovative technique.3. Surgical interventions in the treatment of tubal infertility, when performing reconstructive operations on the fallopian tube, in addition to linear restoration, anastomosis of the fallopian tube requires restoration of its patency, i.e. recanalization of the tube canal along its entire length, sometimes implantation of the isthmus of the fallopian tube into the uterus.4. In the early postoperative period, it is necessary to prevent the formation of adhesions in the pelvis and other preventive measures.
References
| [1] | Kulakov V.I., Volkov N.I., Margiani F.A. Medical and social aspects of women's reproductive health: Abstracts // Sat. scientific proceedings of the plenum of RAAG. -M., 2000. -pp. 121–124. |
| [2] | Gordon D. Tubal infertility. -N.Y., 1996. -pp.145. |
| [3] | Asadov D. A., Vafakulova U. B. Medical and social aspects of infertile marriage // Med. magazine Uzbekistan. - 2004. - No. 4. - pp. 103-105. |
| [4] | Beloborodov S.M. Ciliary dyskinesia in the pathogenesis of tubal infertility // Problems of reproduction. - 2001. - No. 2. - pp. 39-45. |
| [5] | Pshenichnikova T.Ya. Infertility in marriage. -M, 2001. -pp. 318. |
| [6] | Yunda I.F., Ivanyuta L.I., Imshenetskaya L.P. Infertility in marriage. -Kyiv, 1990. -pp.463. |
| [7] | Rowe R.J. Infertility in the family. Fertility regulation today and tomorrow. -N.Y., 1997. -pp. 275-290. |
| [8] | Lockwood C.J., Krikun G., Schatz F. decidual Cell –Expressed tissue Factor Maintains Hemostasis in Human Endometrium // Ann NY Acad Sci. -2001. -Vol. 943. -pp. 77-88. |
| [9] | Polyakova O.V. "Surgical treatment of tubo-peritoneal infertility, prevention of re-formation of adhesions." Diss. Moscow, - 2005. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML