-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(2): 231-236
doi:10.5923/j.ajmms.20241402.14
Received: Jan. 8, 2024; Accepted: Jan. 31, 2024; Published: Feb. 4, 2024

Results of Surgical Treatment of Inguinal Hernia in Elderly and Senile Patients
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKurbaniyazov Zafar Babajanovich, Khamroev G’ulom Abdug’anievich, Nurillaev Khusan Jamshidovich, Rakhmanov Kosim Erdanovich
Samarkand State Medical University, Uzbekistan
Correspondence to: Kurbaniyazov Zafar Babajanovich, Samarkand State Medical University, Uzbekistan.
| Email: |  |
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Studied results surgical treatment 112 patients. An individualized approach to the surgical treatment of inguinal hernias in elderly and senile patients made it possible to reduce the frequency of specific long-term postoperative complications - hernia recurrence from 10.6% in the comparison group to 3.1% in the main group. An improved method of open prosthetic Lichtenstein plastic surgery with strengthening of the anterior and posterior walls of the inguinal canal eliminates the development of recurrent hernia, prevents scrotal swelling in the early postoperative period and is indicated in patients of older age groups with degenerative-dystrophic changes in the tissues of the inguinal region and high (ASA III - IV degree) operational and anesthetic risk. Laparoscopic hernioplasty using the TAPP method is characterized by low-invasiveness, early rehabilitation (reduction of treatment time by 2 times), better quality of life results. The presence of severe comorbid pathology (surgical and anesthetic risk grade III - IV according to ASA) limits its use (32.3% completed) elderly and senile patients.
Keywords: Inguinal hernia, Elderly and senile age, Surgical treatment
Cite this paper: Kurbaniyazov Zafar Babajanovich, Khamroev G’ulom Abdug’anievich, Nurillaev Khusan Jamshidovich, Rakhmanov Kosim Erdanovich, Results of Surgical Treatment of Inguinal Hernia in Elderly and Senile Patients, American Journal of Medicine and Medical Sciences, Vol. 14 No. 2, 2024, pp. 231-236. doi: 10.5923/j.ajmms.20241402.14.
Article Outline
1. Relevance of the Research Topic
- External abdominal hernias occur in 3-4% of the population, and among elderly and senile people - in 15-17%, which undoubtedly leads to a decrease in their quality of life, loss of ability to work and disability [2,10]. Among patients with external abdominal hernias, inguinal hernias account for approximately 80%. To treat them, various surgical methods are used, the number of which today reaches more than 1000, which indicates surgeons’ dissatisfaction with the results of treating this disease [1,4,8,13].Despite the improvement of hernioplasty methods, the percentage of hernia recurrences still remains high, the frequency of which varies according to the literature from 5 to 45% [6,9,12,14]. The introduction of new methods of surgical treatment has led to a significant reduction in the incidence of recurrent inguinal hernia (down to 1-5%). In clinics specifically involved in the diagnosis and treatment of inguinal hernias, the recurrence rate is reduced to a minimum and does not exceed 1-1.5% [3,5,7,11].The reasons for the recurrence of the disease cannot always be clarified, but are often a consequence of the standard use of one or more methods of plastic surgery without taking into account the topography of the groin area, the type of hernia, the age of the patient, and the condition of the tissues.
2. The Purpose of the Study
- To improve the results of surgical treatment of inguinal hernias in elderly and senile patients by optimizing the choice of open prosthetic repair and laparoscopic TAPP hernioplasty.
3. Material and Methods
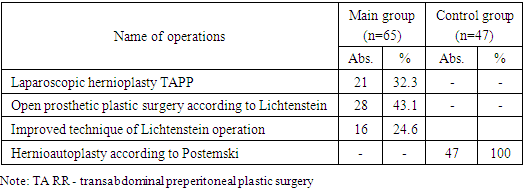
- And learned results _ surgical treatment 112 patients with inguinal hernias seniors age groups hospitalized from 2014 to 2023 in the surgical department of the multidisciplinary clinic of Samarkand State Medical University, being clinical base of the Department of Surgical Diseases No. 1, Transplantology and Urology. IN main group entered 65 sick, at which tension-free prosthetic repair according to Lichtenstein (n = 28) and its improved technique (n = 16), as well as laparoscopic hernioplasty using the TAPP method (n = 21) were used. IN comparison group – 47 sick, at which tension methods were used hernioautoplasty according to Postempsky (n = 47).
|
|
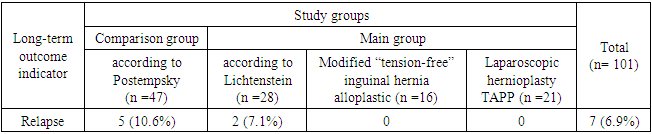
4. Results and Its Discussion
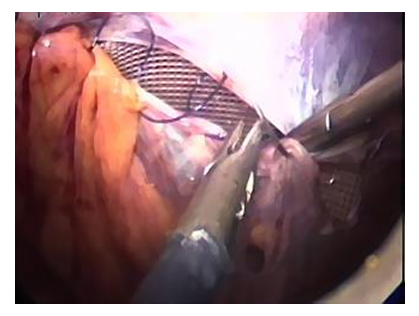
- All patients were operated on as planned. The comparison group consisted of 47 patients with inguinal hernias who underwent hernioautoplasty using the Postempsky method. The main group consisted of 65 patients who underwent “non-tension” inguinal hernia alloplasty using the Lichtenstein method – 28 (43.1%) patients, of which 16 (24.6%) according to our modified method. Also in the main study group, laparoscopic hernioplasty – TAPP (transabdominal preperitoneal plastic surgery) was performed in 21 (32.3%) patients.The “gold standard” for the treatment of inguinal hernia is hernioplasty using the Lichtenstein method. This technique is recommended for use by the European Society of Herniology and is performed through an open access 5-10 cm long, which allows you to eliminate an inguinal hernia of any type and size.However, often the inguinal ligament is so disintegrated that it can hardly be a reliable place for fixing the prosthesis. There is a need for additional fixation. The use of the Cooper ligament for this, as recommended by many authors, only partially solves the problem, and Kozlov’s methods with the formation of an artificial inguinal ligament and Fletching using a “three-layer mesh” are technically complex.In addition, it is not always possible to observe the “no tension” principle with the Lichtenstein technique. The encountered weakness of the inguinal ligament forces, for a more durable fixation of the prosthesis, to resort to gripping part of the aponeurosis of the external oblique abdominal muscle in a continuous suture. In addition, entrapment of the Cooper ligament in the suture displaces the inguinal ligament inferiorly. As a result, suturing flaps of the aponeurosis of the external oblique abdominal muscle is impossible without tension. Even slight tissue swelling that occurs in the postoperative period leads to even greater tension in the anterior wall of the inguinal canal. Incomplete restoration of the integrity of the anterior wall of the inguinal canal, leaving a large external inguinal ring, leads to straightening of the inguinal canal and disruption of its valve function.It should also be noted that exudation arising as a result of surgical trauma and in response to the prosthesis, like a foreign body, can lead to the accumulation of fluid in the cavity of the inguinal canal, swelling of the spermatic cord and testicle. Another important thing is that the posterior wall of the inguinal canal is strengthened only due to the weakened transverse fascia and mesh implant. The mechanical load is immediately placed on the graft. There is a need to use dense “heavy” meshes, because the use of lightweight and semi-absorbable meshes with increased intra-abdominal pressure leads to separation or rupture of the mesh and, as a consequence, recurrence of the hernia. In addition, fixing the upper edge of the graft to the surface of the internal oblique abdominal muscle leads to a number of negative consequences: cutting through the sutures and migration of the mesh implant due to the low mechanical strength of the muscle tissue; to the danger of injury to muscle vessels, and in conditions of early loading - to the formation of intermuscular hematomas, suppuration of the postoperative wound; to the formation of a rough, rigid scar in place of the formed folds.Lichtenstein method in 2 (7.1%) patients observed and reoperated out of 28 patients in the late postoperative period, we found that in both cases the cause of the relapse was the separation of the muscular aponeurotic tissue, the cutting of sutures and migration of a mesh implant under mechanical load in obese patients with high intra-abdominal pressure.Taking into account all the above-mentioned disadvantages and possible complications in the postoperative period, we have developed and introduced into practice an improved “non-tension” inguinal hernia alloplasty. The objective of the proposed method in developing a safe and effective method for the surgical treatment of inguinal hernias was to strengthen the anterior and posterior walls of the inguinal canal through the proposed fixation of a mesh implant, prevent relapses and reduce postoperative complications, early activation and rehabilitation of patients.The “tension-free” inguinal hernia alloplasty we improved was carried out as follows. The skin, subcutaneous tissue and aponeurosis of the external oblique abdominal muscle were dissected according to the generally accepted technique. The hernial sac was isolated and removed or immersed in the abdominal cavity.A mesh implant measuring 10×15 cm was cut intraoperatively, taking into account the individual characteristics of the inguinal space, and plastic surgery of the inguinal canal wall was performed. For this purpose, the upper inner part of the graft was fixed between the lower edge of the transverse muscle and the transverse fascia of the abdomen with U-shaped sutures, and the middle part, by overlapping evenly with straightening the mesh without tension, was fixed to the inguinal ligament with interrupted sutures to a point located 2 cm lateral to the internal inguinal ring (Figure 1).
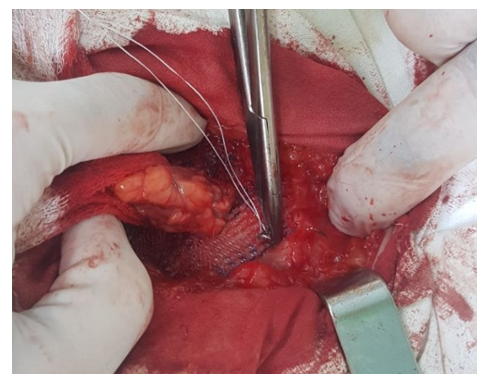 | Figure 1. Fixation of the implant to the upper wall of the inguinal canal |
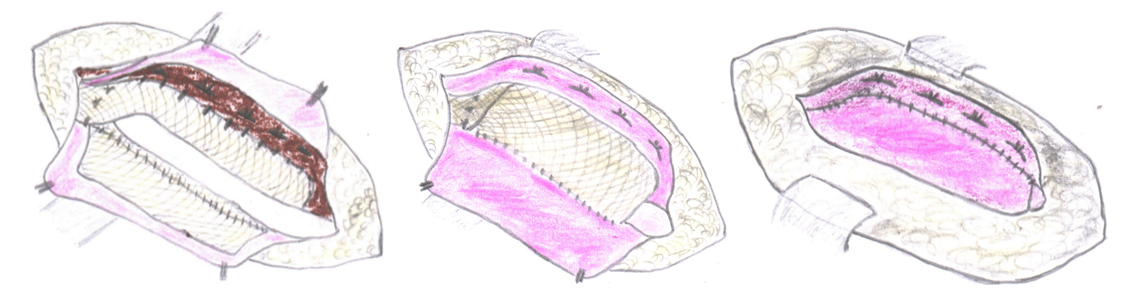 | Figure 2. Stages of performing a modified “tension-free” inguinal hernia alloplasty: a) fixation of the graft with the upper inner part between the lower edge of the transverse muscle and the transverse fascia of the abdomen using U-shaped sutures, and the middle part, by overlapping evenly with straightening the mesh without tension, to the Pupart ligament with interrupted sutures to a point located 2 cm lateral to the internal inguinal ring, the spermatic cord is located above the mesh; b) fixation with U-shaped sutures of the upper outer part of the mesh implant from the inside to the upper flap of the aponeurosis of the external oblique abdominal muscle; c) suturing the edges of the upper and lower flap of the aponeurosis of the external oblique abdominal muscle with interrupted sutures |
 | Figure 3. Final stage. Peritonization of the endoprosthesis |
 | Figure 4. Final stage. Peritonization of the endoprosthesis |
 | Figure 5. Final stage. Peritonization of the endoprosthesis |
|
5. Conclusions
- The choice of inguinal hernioplasty method in patients of older age groups with competing comorbid pathologies should be individualized and based on clarification of surgical and anesthetic risk factors, as well as the type of hernia, the condition of the posterior wall of the inguinal canal and pathological changes in the tissues of the inguinal region. Lichtenstein plastic surgery with strengthening of the anterior and posterior walls of the inguinal canal eliminates the development of recurrent hernia, prevents scrotal swelling in the early postoperative period and is indicated in patients of older age groups with degenerative-dystrophic changes in the tissues of the inguinal region and high (ASA III - IV degree) operational and anesthetic risk. Laparoscopic hernioplasty using the TAPP method is characterized by low trauma, early rehabilitation (reduction of treatment time by 2 times), and better quality of life results. The presence of severe comorbid pathology (surgical and anesthetic risk grade III - IV according to ASA) limits its use (32.3% performed) in elderly and senile patients. An individualized approach to the surgical treatment of inguinal hernias in elderly and senile patients made it possible to reduce the frequency of specific long-term postoperative complications - hernia recurrence from 10.6% in the comparison group to 3.1% in the main group.Information about the source of support in the form of grants, equipment, and drugs. The authors did not receive financial support from manufacturers of medicines and medical equipment.Conflicts of interest: The authors have no conflicts of interest.