-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(2): 208-211
doi:10.5923/j.ajmms.20241402.09
Received: Jan. 15, 2024; Accepted: Jan. 29, 2024; Published: Feb. 4, 2024

Assessment of Providing Medical Care in Cases of Obstetric Bleeding in the Republic of Karakalpakstan
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLG. A. Seyfullaeva1, O. I. Khvan2, F. D. Karimova3
1Doctoral Student at the Scientific and Practical Center for Forensic Medical Examination of the Ministry of Health of the Republic of Uzbekistan, Tashkent, Uzbekistan
2Deputy Director for Scientific Work of the Scientific and Practical Center for Forensic Medical Examination of the Ministry of Health of the Republic of Uzbekistan, Tashkent, Uzbekistan
3Head of the Department of Obstetrics and Gynecology of the Center for Professional Qualification of Medical Workers of the Ministry of Health of the Republic of Uzbekistan, Tashkent, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

An analysis of the causes of obstetric bleeding is described on the basis of examinations received from all regions of the Republic of Karakalpakstan to the department of repeated examination of the state of maternal mortality. The most important reasons for the development of negative consequences in obstetric and gynecological practice have been identified. Deficiencies in the organization, diagnosis and treatment and their relationship with the occurrence of unpleasant consequences are revealed.
Keywords: Obstetric bleeding, Maternal mortality, Medical care
Cite this paper: G. A. Seyfullaeva, O. I. Khvan, F. D. Karimova, Assessment of Providing Medical Care in Cases of Obstetric Bleeding in the Republic of Karakalpakstan, American Journal of Medicine and Medical Sciences, Vol. 14 No. 2, 2024, pp. 208-211. doi: 10.5923/j.ajmms.20241402.09.
1. Relevance
- The relevance of this topic lies in the fact that obstetric hemorrhage has long been one of the leading causes of maternal morbidity and mortality in the world. According to WHO, 14,000,000 postpartum hemorrhages occur annually in the world, of which 120,000-140,000 cases result in death and 2,000,000 cases result in illness in women. Direct causes of maternal mortality (up to 80%) can be prevented with timely and appropriate care. Maternal mortality is primarily associated with bleeding. A meta-analysis of a cohort of women with bleeding shows the importance of certain risk factors. [1]The World Health Organization (WHO) defines maternal mortality as “the death of a woman during pregnancy or within 42 days after childbirth from any cause related to pregnancy, aggravated by its management, but not from accidental or accidental causes.” [2-6]The provision of perinatal care in our country is carried out on the basis of the order of the Ministry of Health of the Republic of Uzbekistan, which has a 3-level structure, No. 185 of 2014 “On the territorialization of perinatal care in Uzbekistan”, pregnant women of a dangerous category should be transferred to 3rd level medical care institutions level. Many studies demonstrate the effectiveness of rational regionalization and targeting of perinatal care for high-risk pregnant women in reducing maternal mortality and morbidity. [7-11]Timely referral and transfer of high-risk women to perinatal centers with conditions for multidisciplinary care, adequate equipment, good infrastructure and laboratory, timely diagnosis of critical (severe) conditions and rational therapy to prevent maternal mortality. [12-15]
2. Purpose of the Study
- The Republican Scientific and Practical Center for Forensic Medical Examination of the Ministry of Health of the Republic of Uzbekistan in the branch in the Republic of Karakalpakstan will have to analyze the examination of the commission related to the provision of obstetric care in the period 2017-2022. Medical documents were analyzed (outpatient records, personal records of pregnant women and women in labor, birth histories, developmental histories of newborns, reports of pathological examinations, protocols of office examinations and clinical-anatomical conferences, examinations of the corpse). and expert opinions of the commission, materials of investigation and criminal cases) in order to establish the causes of shortcomings in the provision of medical care at various stages of prevention, organization, diagnosis and treatment, unfavorable results were recorded in the provision of obstetric and gynecological care. gynecological care for 51 patients.
3. Research Results
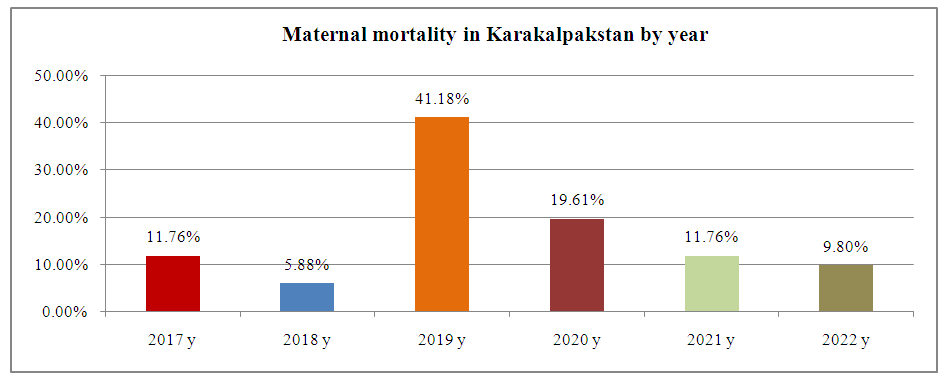
- During the period 2017-2022, the total number of medical examinations carried out in the Republic of Karakalpakstan in connection with the provision of medical care to pregnant women and maternal mortality was 6 (11.76%) in 2017, 3 (5.88%) in 2018, 21 ( 41.18%) in 2019. 10 (19.61%) in 2020, 6 (11.76%) in 2021, 5 (9.8%) in 2022. This indicator shows the highest result in 2019. (Figure 1)
 | Figure 1 |
 | Figure 2 |
 | Figure 3 |
 | Figure 4 |
4. Conclusions
- When conducting examinations related to the correct provision of obstetric and gynecological care, the expert commission found that in 90% of cases, the shortcomings of diagnostic and treatment tactics are not only the objective difficulties of diagnosis, but also the lack of assessment of the severity of the disease. the patient's condition, lack of timely and complete examination, lack of timely detection of the underlying disease and complications, lack of dynamic observation, incorrect choice of delivery tactics, incorrect assessment of the volume of lost blood, it was found that the volume of lost blood was not filled in on time and completely.Complications during pregnancy caused severe complications.Most of the shortcomings in diagnostic and therapeutic care are due to the lack of an individual approach to the patient.In most cases, observed deficiencies in obstetric and gynecologic care are not causally related to adverse pregnancy or childbirth outcomes, but have a significant impact on outcomes and contribute to adverse outcomes.The study revealed that more than 70% of the population contacted the district medical association. This is due to the provision of medical care in the District Medical Association with high-quality conditions, sufficient equipment, good infrastructure and laboratory, and the work of our qualified medical operators contributes to the timely prevention of bleeding.