-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(1): 79-82
doi:10.5923/j.ajmms.20241401.18
Received: Dec. 19, 2023; Accepted: Jan. 8, 2024; Published: Jan. 12, 2024

Assessment of Essential Microelements Deficiency in Different Stages of Chronic Kidney Disease
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRajabov N. M., Akhmedova N. Sh.
Bukhara State Medical Institute, Bukhara, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Chronic kidney disease (CKD) is one of the most common diseases among the population of the earth, and is the leading cause of death and disability. Risk factors causing CKD are widespread, among which the role of vital micronutrients is very important. This research paper presents the results of the study of zinc, copper and iron trace elements deficiency in patients in the early stages of CKD and their clinical course. The results showed that correlations were found between disease stages and micronutrient deficiency.
Keywords: Chronic kidney disease, Zinc, Copper, Trace elements
Cite this paper: Rajabov N. M., Akhmedova N. Sh., Assessment of Essential Microelements Deficiency in Different Stages of Chronic Kidney Disease, American Journal of Medicine and Medical Sciences, Vol. 14 No. 1, 2024, pp. 79-82. doi: 10.5923/j.ajmms.20241401.18.
1. Introduction
- Although many achievements have been achieved as a result of the research carried out in the world, many questions in the field of diagnosis and prevention of CKD of social importance in practical medicine have not yet been resolved. [4,6].In recent years, research aimed at studying the problem of the development of micronutrients shows that the relevance of this problem is related to a number of factors called the biogeochemical state. These factors are related to ecological, anthropogenic and climatic geographical features, which have a permanent effect on the human body. [1-5]. In the study of the problem, it was found that a lot of scientific research work has been carried out on the determination and correction of micronutrient status in the terminal stage of chronic kidney disease, and information on micronutrients in the II-III stages of the disease and in the period before dialysis is very rare. At the same time, kidney failure, which is important for maintaining the homeostasis of the body, causes a change in the micronutrient status and an increase in the development of the disease, an increase in complications from the cardiovascular and digestive systems. [1,2,3,6].Today, among the population of the earth, the number of people with chronic kidney failure is continuously increasing [1,5,7,9]. CKD takes one of the leading places among chronic non-infectious diseases, occurring from 6% to 20% in different countries. Also, in many cases, due to the fact that patients need expensive replacement therapy (dialysis or kidney transplantation), the quality of life decreases, disability and death are high. [6,8,10].CKD is a collective expression indicating damage to kidney tissue regardless of etiological origin. The presence of any marker of kidney damage (albuminuria/proteinuria, pathological deposits in the urine, morphological changes) for three months or more, or a glomerular filtration rate (GFR) <60 ml per minute per 1.73 m2 of body surface area for the same period is considered CKD. The concept of CKD was developed in the clinical recommendations of the international organization Kidney Disease: Improving Global Outcomes (KDIGO) [4,11].The purpose of this research workis to assess the diagnostic and prognostic effectiveness of early detection of essential micronutrient deficiency in patients with various stages of chronic kidney disease development.
2. Materials and Methods
- 180 patients aged 18-60 with different levels of CKD were included in the study. 41.1% of patients (n=74) men and 59.9% (n=106) were formed by women. The average age of patients is 48.3±equal to 1.4. In order to assess kidney function, serum creatinine, cystatin, urea, BKFT, and renal reserve indicators were studied in all patients. Also, the amount of essential microelements iron, copper and zinc was studied by clinical analysis and IFA method.Statistical processing of the obtained data was carried out by calculating the following parameters: arithmetic mean (M), arithmetic mean error (m), confidence interval. Differences between indicators were considered significant when the probability level was r < 0.05.
3. Analysis of Results
- At the initial stage of the scientific research work, the risk factors causing CKD were studied in the patients involved. It was based on the patient's anamnesis, past illnesses, genetic anamnesis, objective and subjective examination results (Fig. 1).
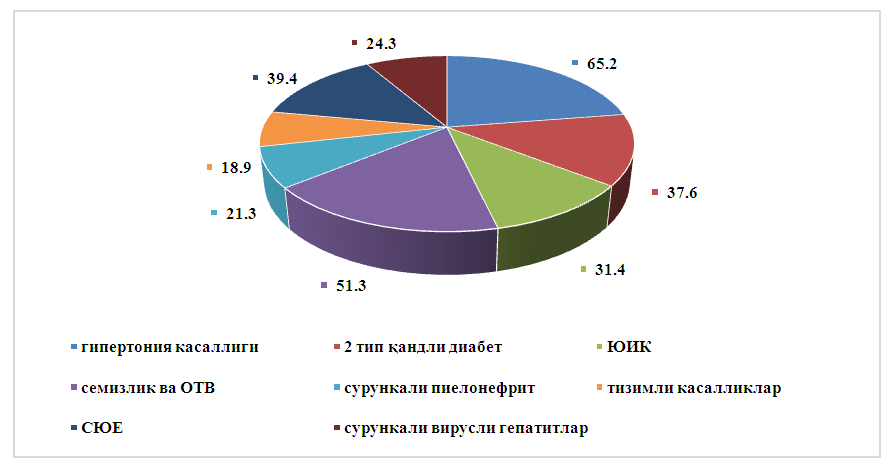 | Figure 1. Frequency of occurrence of risk factors causing CKD (%) |
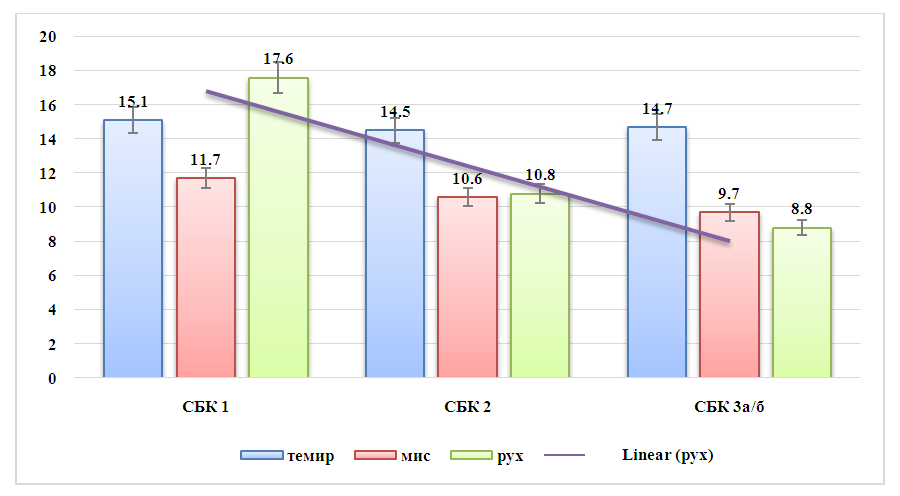 | Figure 2. The status of the development of essential micronutrient deficiency with the CKD stages (in men) |
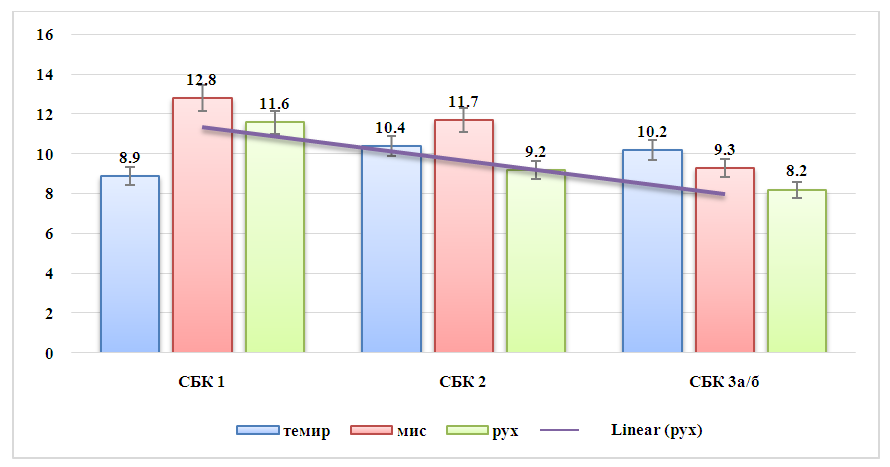 | Figure 3. The relationship between the development of essential micronutrient deficiency and the stages of CKD (in women) |