-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(1): 46-48
doi:10.5923/j.ajmms.20241401.11
Received: Dec. 20, 2023; Accepted: Jan. 5, 2024; Published: Jan. 8, 2024

Evaluation of Clinical-Laboratory Severity Levels of Irritable Bowel Syndrome
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMakhmudova L. I., Abdullayev I. A.
Bukhara State Medical Institute named after Abu Ali ibn Sina, Bukhara, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

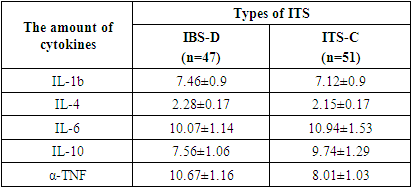
The study was conducted in the department of polyclinic and gastroenterology of the Bukhara Regional Multidisciplinary Medical Center and selected 98 patients who underwent outpatient examination with irritable bowel syndrome (IBS). Patients with IBS were divided into two groups: IBS with a predominance of diarrhea (patient IBS-D-47) and IBS with a predominance of constipation (patient IBS-C-51). Intestinal symptoms were more pronounced in the type of IBS with a predominance of diarrhea compared to the type of IBS with a predominance of constipation. When comparing the types with a predominance of diarrhea and constipation in terms of the severity of the clinical course of the disease, severe course was noted in 14.9% of patients with IBS-D and in 27.4% of patients with IBS-C.
Keywords: Irritable bowel syndrome, Intestinal symptoms, Cytokines, Fecal calprotectin
Cite this paper: Makhmudova L. I., Abdullayev I. A., Evaluation of Clinical-Laboratory Severity Levels of Irritable Bowel Syndrome, American Journal of Medicine and Medical Sciences, Vol. 14 No. 1, 2024, pp. 46-48. doi: 10.5923/j.ajmms.20241401.11.
1. Introduction
- Irritable bowel syndrome (IBS) is a biopsychosocial disease consisting of a set of functional disorders not explained by organic changes in the intestines [1,4,5].The analysis of modern data on the etiology and pathogenesis of the functional pathology of the digestive tract allows us to comment on the concept of the formation of the disease, which, of course, is not one, but several etiological factors, and these factors, in turn, are not the same. Rather, it is related to several pathophysiological mechanisms. And the complexity of controlling such patients is that the combination of etiopathogenetic mechanisms in each individual case is individual. Among them, the following are relevant today: socio-economic status, genetic predisposition, the probability of the disease in children of parents with IBS, psychological aspects, hypersensitivity of internal organs, disorders of the gastrointestinal tract, neuroendocrine system changes (brain-intestinal axis), low-grade inflammation, the concept of IBS after an infectious disease, microflora imbalance and finally, nutritional factors [2,3,6,7].The purpose of the study consists in evaluating the clinical-laboratory severity levels of the disease in the types of irritable bowel syndrome with the predominance of diarrhea and constipation.
2. Material and Methods
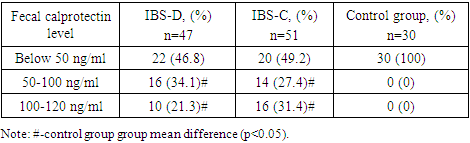
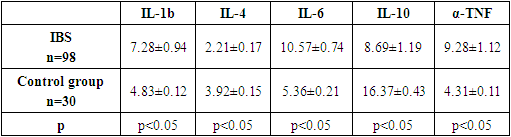
- The study was conducted in the polyclinic and gastroenterology department of the Bukhara regional multidisciplinary medical center (BRMDMC), and 98 patients who were examined with IBS in outpatient conditions were selected. The diagnosis of IBS was made based on IV Rome criteria (2016). The average age of patients is 34.6±0.9 years.Patients with IBS were divided into two groups: IBS type with diarrhea predominance (IBS-D – 47 patients) and constipation type with predominance (IBS-C – 51 patients).All patients underwent general blood, general fecal analysis, fecal occult blood test, blood biochemical analysis, intestinal microbiota analysis, cytokine analysis - IL-1 b, IL-4, IL-6, IL-10, α-TNF (Vekor-Best reagents), fecal calprotectin (De medi tec reagents) and cortisol analysis in blood, from instrumental examinations - esophagofibromastroduodenoscopy (FUGINON. FUGI FILM EPX-2500, 2014, Japan; FUGI FILM-EG-530PF, 2014, Japan), colonoscopy (FUGI FILM-EG -530FL, 2014, Japan), ultrasound examination of internal organs (Vivid S-60, 2014, Norway) was performed.
3. Results and Analyses
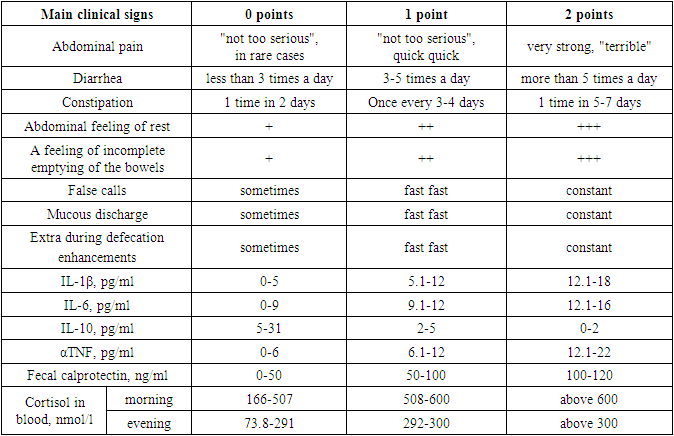
- After patients with an IBS-like syndrome were excluded from the study, 98 patients diagnosed with IBS were included in the follow-up program.30 healthy subjects were included in the control group to obtain normative data. The average age of the control group was 29.3±1.02 years. The study was carried out simultaneously. The type of clinical course of IBS was determined clinically, as well as retrospectively, taking into account the anamnesis data and the results of the study of medical records.In order to facilitate the examination and data analysis, a program was developed for the assessment of symptoms: absence of symptoms 0 points, mild to moderate symptoms - 1 point, severe symptoms - 2 was evaluated with points. The points collected by each patient are based on clinical-laboratory symptoms (abdominal pain, diarrhea, constipation, feeling of abdominal rest, feeling of incomplete bowel emptying, false stools, mucus discharge, defecation additional increases in time, IL-1β, IL-6, IL-10, αTNF, cecal calprotectin and blood cortisol) were summarized. Patients with a score of 21-28 were considered to have a severe disease, patients with a score of 10-20 were considered to have a moderate disease, and patients with a score of 1-9 were considered to have a mild disease (Table 1).
|
|

|
|
|
|
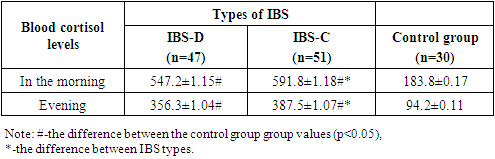
4. Conclusions
- Thus, when analyzing the types of bowel syndrome with the predominance of diarrhea and constipation according to clinical and laboratory parameters, the main part of the patients was mild. At the same time, an increase in the amount of inflammatory cytokines and cortisol in the blood also requires an individual approach to the selection of treatment methods.