-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2024; 14(1): 7-9
doi:10.5923/j.ajmms.20241401.02
Received: Dec. 5, 2023; Accepted: Dec. 27, 2023; Published: Jan. 3, 2024

Morphological Features of Fat Embolism in Fractures of Tubular Bones
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSukhrob Sultanov, Ibragim Bakhriev
Tashkent Medical Academy, Uzbekistan
Copyright © 2024 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article covers a problem of a fatty embolism as a heavy complication of a mechanical trauma that often can be cause of death of the victim or playing a fundamental role in a thanatogenesis. The article briefly clears up the questions of an etiology and pathogenesis, clinical diagnostics and generally touches on an issue of morphological (primary – microscopic) diagnosis of a fatty embolism.
Keywords: Fat embolism, Fractures of bones, Morphology of a fatty embolism, Traumatic illness
Cite this paper: Sukhrob Sultanov, Ibragim Bakhriev, Morphological Features of Fat Embolism in Fractures of Tubular Bones, American Journal of Medicine and Medical Sciences, Vol. 14 No. 1, 2024, pp. 7-9. doi: 10.5923/j.ajmms.20241401.02.
1. Introduction
- Contrary to expectations, the progressive developments of society and scientific-technical progress have not led to a decrease in trauma in the 21st century. Moreover, according to foreign and domestic literature, there has been incessant increase in severe trauma in the structure of diseases leading to long-term disability and disability in patients. According to the World Health Organization, trauma ranks third in terms of frequency and overall mortality in the population. Trauma, as a cause of mortality, is the leading one in the age group from 20 to 60 years, exceeding it by two times the combined number of cardiovascular and oncological diseases [1]. The average age of patients with polytrauma is 38.5 years [2].A severe complication in the early stages of trauma that increases lethality is fat embolism. However, clear understandings of the pathogenesis, clinical presentation, prevention, and treatment of fat embolism are still lacking. The frequency of fat embolism development varies, according to different authors, from 0.5 to 30% in injuries involving multiple fractures of long tubular bones and fractures of the pelvic bones. Despite intensive modern therapy, the mortality rate ranges from 3 to 67% [3-5].Fat embolism occurs due to the entry into the blood of droplets of either endogenous or exogenous neutral fat. Causes of this include skeletal trauma (closed fractures or gunshot wounds of long tubular bones, multiple rib fractures, pelvic bone fractures), extensive soft tissue injuries with crushing of subcutaneous adipose tissue, severe burns, intoxication or electrical injuries, hepatic fat dystrophy, closed heart massage, and certain types of anesthesia. Fat embolism can also occur when administering oil-based therapeutic or diagnostic preparations to patients. Fatty droplets usually enter the lungs and get trapped in small blood vessels and capillaries. Some fat droplets pass through arteriovenous anastomoses into the systemic circulation and are disseminated by blood to the brain, kidneys, and other organs, blocking their capillaries. At the same time, there are no macroscopic changes in the organs. However, targeted examination of histological specimens using fat-revealing dyes allows for the diagnosis of fat embolism in most similar situations.Due to the complexity of clinical diagnosis and the lack, in most cases, of reliable macroscopic signs indicating its presence, fat embolism is often overlooked in autopsies of individuals who died from mechanical injuries. This, in general, reduces the quality of the conducted examinations. The aim of the research is to assess the level of fat embolism in blood vessels by staining pieces of internal organs of the corpse with Sudan III dye for histological examination, with the purpose of determining the primary cause of death in fractures of long tubular bones.
2. Materials and Methods
- The material for the study consisted of 36 histological specimens prepared from the internal organs of a corpse that was admitted to the hospital with a combined severe trauma during its lifetime. The prepared specimens are stained with hematoxylin-eosin and Sudan III dye for further examination.To identify lipid inclusions from lung tissue fixed for no more than two days in a 10% formalin solution, thin slices of lung tissue were made using a freezing microtome. These sections were placed on glass slides, stained with Sudan III, then with hematoxylin, covered with glycerin, and a cover slip was applied, the edges of which were secured with a mounting medium. Simultaneously, some pieces of lung tissue were embedded in paraffin, and the sections were stained with hematoxylin and eosin.When stained with hematoxylin and eosin, small round-to-oval optical voids resembling fat emboli were found in the lumens of various-sized vessels in all cases. The presence of fat emboli was assessed on Biolam-L-1 and XS 90 microscopes on a section area of 2 square centimeters. When stained with Sudan III, fat emboli were found in vessels of various calibers, appearing as rounded obtrusive forms that filled the entire vessel lumen and sausage-shaped homogeneous droplets of orange-yellow color.
3. Results and Discussion
- Internal organs subjected to histological examination included the brain, heart, lungs, and kidneys.Brain (cortex): The soft meningeal membrane is thin, with venous-venular congestion and brain substance; pronounced perivascular edema, dystrophic changes in neurons throughout the sections. When stained with Sudan III, more than 10 fat emboli were found in vessels in 10 fields of view and with a microscope magnification of 7x8 (Figure 1).
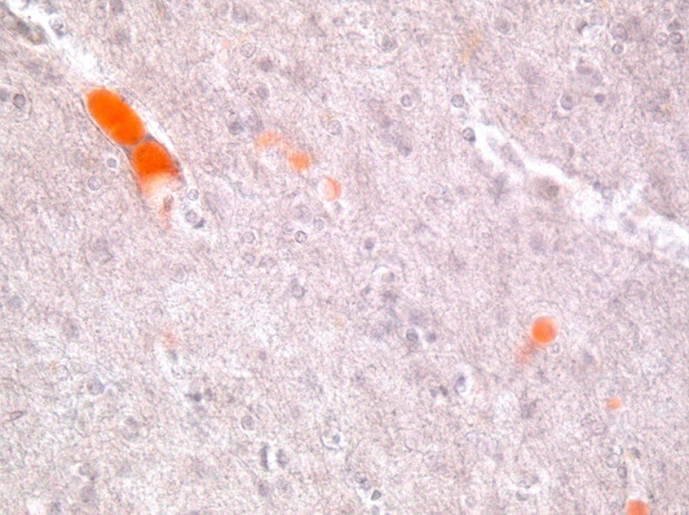 | Figure 1. Brain. Orange-colored fat emboli in the lumen of capillaries. Staining with Sudan III, magnification x400 |
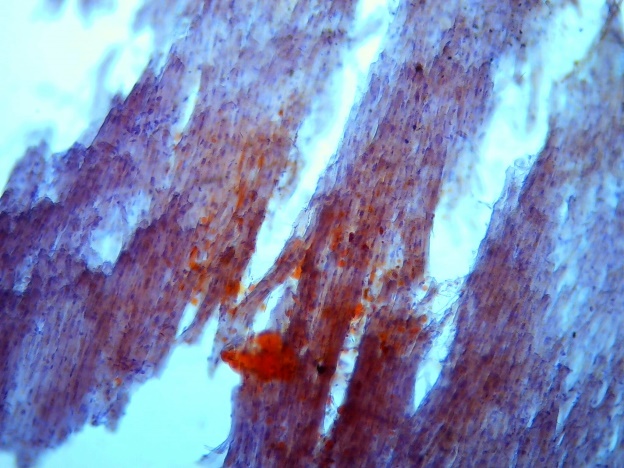 | Figure 2. Heart. Orange-colored fat emboli in the lumen of capillaries. Staining with Sudan III, magnification x100 |
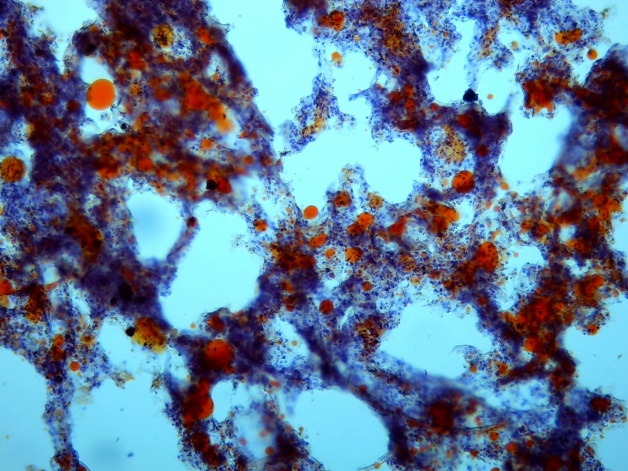 | Figure 3. Lungs. Orange-colored fat emboli in the lumen of arterioles. Staining with Sudan III, magnification x100 |
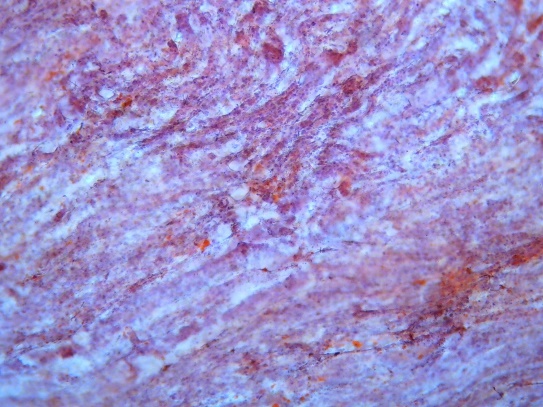 | Figure 4. Kidney. Cortical layer. Orange-colored fat emboli in the capillaries of glomeruli. Staining with Sudan III, magnification x200 |
4. Conclusions
- The particular feature of this study is the identified fat embolism in the brain, lungs, heart, and kidneys, of a significant degree, during forensic-histological examination. This fat embolism was determined to be the immediate cause of death in the case of a mechanical injury with multiple fractures of long bones. The source of fat embolism in this case was the adipocytes, which are consistently present in the red bone marrow of long tubular bones. It is also significant that blunt force always creates conditions for traumatizing subcutaneous adipose tissue and blood vessels, leading to the formation of fat embolism in the pulmonary vessels of varying degrees (often minor). The fact that primary fat droplets in the bloodstream induce the phenomenon of lipid demulsification and become centers of their aggregation is also noteworthy.