-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2023; 13(12): 2072-2077
doi:10.5923/j.ajmms.20231312.55
Received: Dec. 19, 2023; Accepted: Dec. 29, 2023; Published: Dec. 30, 2023

Efficacay оf Rosuvastatin and Prendiprol/Amlodepin Single-Pill Combination in Hybpertension Patients with Comorbid Conditions in Patients with Cardiovascular Diseases in Uzbekistan
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLOybek Urinov Urinovich, Abidova Dilorom Ergasheva
Republican Specialized Scientific and Practical Medical Center of Cardiology, Tashkent, Uzbekistan
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

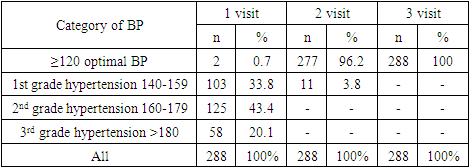
Background: The aim of this study is to evaluate the clinical efficacy of single-pill combination of perindopril/amlodipine and a tablet of rosuvastatin in comorbid conditions in patients with cardiovascular diseases with risk factors in outpatient settings. Material and Methods: 288 patients with stable coronary heart disease (CHD) and hypertension who applied for a consultation at the Republican Specialized Scientific and Practical Medical Center for Cardiology in Tashkent were included. Results: For 3 months, 288 patients with coronary heart disease and hypertension were observed, including 190 (66.0%) men and 98 (34.0%) women. The average age of the population was 58.35±8.57 years, incl. men - 57.13±8.76 years, women - 60.74±7.71 years. 43.75% of patients had overweight and/or obesity, the frequency was similar among both men and women (40.5 % and 50.0% respectively). The initial level of SBP/DBP averaged 161.65±17.99/97.05±10.29 mm Hg, after a month treatment with perindopril/amlodipine SPC in dosage range from 4/5 mg to 8/10 mg the level of blood pressure decreased by 37.58±10.61/18.85±3.97 mm Hg (p<0.0001). At the end of the study all patients achieved target BP. Treatment of hyperlipidemia with rosuvastatin in dosage range from 5 mg to 30 mg in patients with CHD reduced the level of total cholesterol by 75.27±20.69 mg/dL, triglycerides by 45.35±20.02 mg/dL, LDL by 51.45±15, 55 mg/dL, and increased HDL-C up to 5.75 ± 3.9 mg/dL. Conclusions: Therapy of hypertension with perindopril/amlodipine SPC across the whole range of strengths is effective and safe and led to target BP levels at the end of the study in 96.2% of patients with CHD. The therapy of hyperlipidemia with rosuvastatin across the whole range of strengths was evaluated as effective and safe, however the more stringent use of higher strengths of rosuvastatin would provide lower LDL-C levels in very high risk patients with CHD.
Keywords: Perindopril/amlodipine, Rosuvastatin, Cardiovascular disease, Hypertensive patients
Cite this paper: Oybek Urinov Urinovich, Abidova Dilorom Ergasheva, Efficacay оf Rosuvastatin and Prendiprol/Amlodepin Single-Pill Combination in Hybpertension Patients with Comorbid Conditions in Patients with Cardiovascular Diseases in Uzbekistan, American Journal of Medicine and Medical Sciences, Vol. 13 No. 12, 2023, pp. 2072-2077. doi: 10.5923/j.ajmms.20231312.55.
1. Introduction
- The data of long-term monitoring of the incidence and its dynamics in different countries show that cardiovascular diseases (CVD), especially coronary heart disease (CHD) and stroke, are the main causes of death and disability in the middle-aged population [1]. Despite the progress made in recent years in prevention and treatment of CHD, still occupies a leading position in the structure of morbidity and mortality in the population.According to the World Health Organization (WHO), 17.9 million people died from CVDs in 2019, representing 32% of all global deaths. Of these deaths, 85% were due to heart attack and stroke [2].CVD are the number one cause of death also in countries of Central Asia. The high burden of these conditions usually results from insufficient preventive care and lack of education about the prevention and treatment of these diseases. The mortality from CVD in Central Asia countries is generally higher than that in Europe, representing a heavy burden for society with severe socio-economic consequences [3]. Uzbekistan registers more than 1.5 million acute and chronic CVD cases on an annual basis, with more than half a million of them being newly diagnosed [3]. With incidence of 1,493 per 100,000 inhabitants, Uzbekistan has one of the highest incidence of CVD among WHO European Region Member States [4]. Among all leading causes of the overall morbidity in Uzbekistan, 40.4% is occupied by diseases characterized by an elevated blood pressure, including hypertension with target organ damage (14.2%), angina (7.7%), chronic ischemic disease heart disease (7.0%), cerebrovascular disease (4.1%) and acute myocardial infarction (0.54%) [3]. This goes along with high blood pressure being on first place, and high LDL-C on sixth place among risk factors that contribute the most in death and disability combined in Uzbekistan [5].Despite overwhelming evidence that arterial hypertension (AH) and hypercholesterolemia (HCL) are the major CV risk factors and that BP and lipid-lowering treatment strategies substantially reduce the CV risk the rate of BP and LDL-C control remains low worldwide [6-8]. Arterial hypertension is one of the most significant modifiable risk factors for the development of cardiovascular diseases (CVD). Being the basis of the cardiovascular (CV) continuum, hypertension causes a number of causal relationships that adversely affect the risk of developing both major CVDs and their complications, which together becomes a due to its high prevalence in the population and severe socio-economic consequences [3].The CV protection by antihypertensive treatment substantially depends on BP lowering per se. Pharmacological therapy has pivotal role in the management of arterial hypertension. Most patients require ≥ 2 antihypertensive agents from complementary classes to achieve BP control, with renin-angiotensin system (RAS) blockers (angiotensin II receptor blockers (ARBs) or angiotensin converting enzyme inhibitors (ACEi)), calcium channel blockers (CCB) and diuretics being the first-line options). Moreover, combination therapy, preferably in form of single-pill combination (SPC), is a preferred first-line therapy in the majority of patients, as recommended by 2018 ESC/ESH guidelines for the management of arterial hypertension. Such an approach is expected to double BP control rates [7]. However, achieving and maintaining the target level of blood pressure remained an unresolved problem in cardiology and hypertension throughout the world. Despite a number of proven, highly effective and well-tolerated drug treatment strategies, BP control rates remain poor, with only 35% of patients with controlled BP of <140/90 mm Hg. The inability to achieve better BP control is attributed to several reasons, such as physician inertia, patient adherence to the treatment, insufficient use of combination treatment and complexity of treatment strategy [7].Hypertension rarely occurs in isolation, and often clusters with other CV risk factors such as hypercholesterolemia (HCL). This metabolic risk factor clustering has a multiplicative effect on CV risk [7]. More than 60% of hypertensive patients are consistently hypercholesterolemic and the combined diagnosis and optimal management of both risk factors in clinical practice is still poor mainly due to short duration of therapy, poor adherence, despite the fact that treatment of hypertension and hyperlipidemia should be lifelong [9,10].According to published data, less than 50% of treated patients achieve target office BP and only 33% of treated patients achieve target LDL-cholesterol. According to recently published Da Vinci study in secondary prevention patients, the achievement of target LDL-C is even lower, 18% [11,12]. Current 2019 ESC/EAS Guidelines for the management of dyslipidaemias recommend a high-intensity statin (e.g. rosuvastatin) is prescribed up to the highest tolerated dose to reach the LDL-C goals set for the specific level of CV risk. If the goals are not achieved with the maximum tolerated dose of a statin, combination with ezetimibe is recommended. In patients with CHD, LDL-C should be lowered to 1,4 mmol/L (54 mg/dL) and ≥50% reduction should be achieved according to guidelines [8].The development of CHD is accompanied by a high incidence of hospital deaths and non-fatal CV 0complications. The leading role in the development of which is played by risk factors, especially their combinations, which potentiates the possibility of developing the disease and its outcome depending on the number of risk factors. Overweight and obesity reduce human life expectancy by an average of 8 - 11 years. In recent years, the prevalence of this condition has increased significantly in developing countries. It is also important that the potential of each risk factors may have regional characteristics. In Uzbekistan, almost half of adults are overweight, with prevalence of 48.9% in women and 47.3% in men. The prevalence of obesity in Uzbekistan is higher than the regional average [13]. Information on the prevalence and management of AH and HCL and concomitant risk factors are mainly derived from data in Europe and USA, and the information on such data for Uzbekistan are scarce. Therefore, any information on management of CV risk factor in Uzbekistan is valuable. The INTERIM results of ongoing DISCOVERY international epidemiological study that was conducted also in Uzbekistan, in which re-examination of Uzbek patients with hypertension and/or hyperlipidemia revealed, that 96,9 % had both CV factors, hypertension and hyperlipidemia [14].Below we are presenting the valuable data from Synergy study, conducted in Uzbekistan. The aim of the study was to evaluate the clinical efficacy of rosuvastatin (Roswera, Krka d. d. Novo mesto) and single pill combination (SPC) perindopril/amlodipine (Amlessa, Krka d. d. Novo mesto) in comorbid conditions in patients with CVD with risk factors in outpatient clinic 2.
2. Results
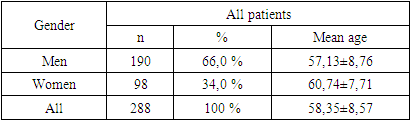
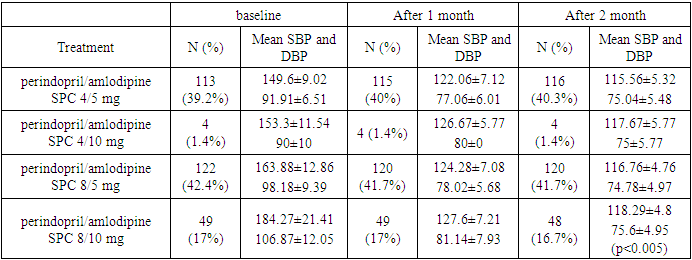
- 288 patients with CHD and AH were observed over the course of 3 months. 66% (190) were men and 34% (98) women (p = 0.0001). The average age of patients was 58.35±8.57 years.
|
|
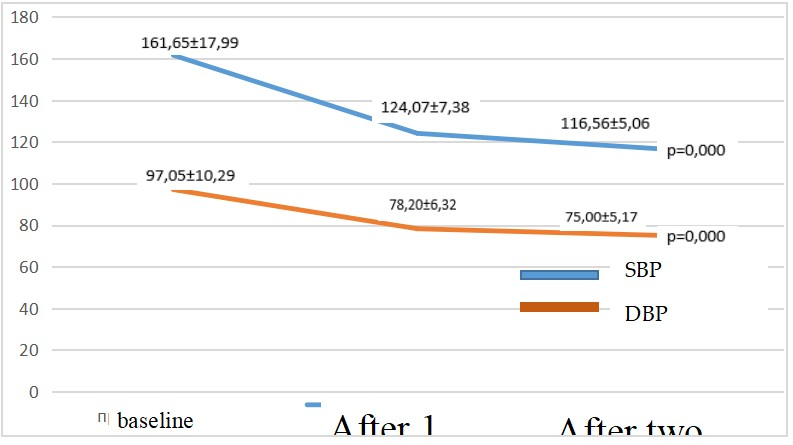 | Figure 1. Office blood pressure levels and changes after 2 months by treatment regimen SPC perindopril/amlodipine |
|
|
|
|
3. Discussion
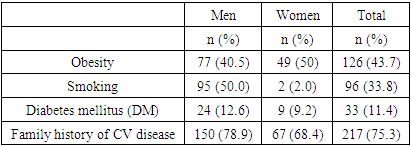
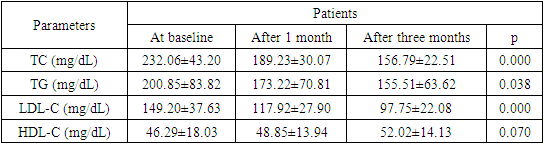
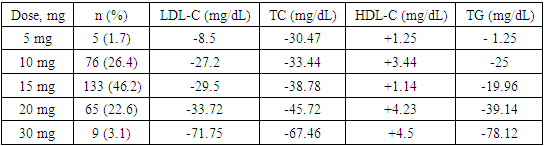
- The need to lower blood pressure (BP) in AH is of paramount importance for the effective lowering of CV risk, especially in very high-risk patients with CHD. A large meta-analysis of prospective and descriptive studies showed, that a decrease in SBP of only 2 mm Hg leads to a decrease in the risk of death from CHD by 7%, death from cerebral stroke by 10%. A decrease in SBP by 20 mm Hg diastolic (DBP) at 10 mm Hg provides a 2-fold reduction in CV mortality [15].The analysis of the prevalence of risk factors in Synergy study showed that obesity was detected in 126 patients (43.75 %), 96 (33%) of patients smoked and 33 (11.4 5%) of patients suffered from DM, which was 1.4 times more often in men than women.The results of our study are generally consistent with the literature data. In our study, treatment of hypertension with perindopril/amlodipine SPC proved to be effective in hypertensive patients at very high risk. The initial level of SBP/DBP at baseline was in average 161.65±17.99 / 97.05±10.29 mm Hg and after 1 month of perindopril / amlodipine SPC, decreased by 37.58 ± 10.61/18.85 ± 3.97 mm Hg (p<0.0001) to optimal 125.07±7.38/78.20±6.32 mm Hg. After 2 months, it decreased for SBP/DBP by 45.09±12.93/22.05±5.12 mm Hg, which theoretically provides a 4-fold reduction in CV mortality. According to our data, the SPC of perindopril/amlodipine effectively controls peripheral BP during the day. The ASCOT-BPLA study (The AngloScandinavion Cardiac Outcomes Trial-Blood Pressure Lowering Arm) [16] involved 19,342 patients with hypertension and other CV risk factors (3 or more), comparing two treatment strategies: perindopril + amlodipine and β blocker atenolol + diuretic. In the group of therapy based on the combination of perindopril + amlodipine, there was a significant reduction in the risk of CV complications compared with treatment with atenolol + diuretic: a decrease in CV mortality by 24%, stroke - by 30%, impaired renal function - by 15%, the total number of CV events and revascularizations by 16%. An important feature of the combination of perindopril and amlodipine is the effective reduction of not only peripheral, but also central blood pressure, as shown in the CAFE (Conduit Artery Function Evaluation) study - ASCOT sub-study [17]. This feature is of great clinical importance, since an increase in central blood pressure and central pulse pressure increases the risk of stroke, myocardial ischemia, and left ventricular hypertrophy.Epidemiological studies among patients with arterial hypertension clearly demonstrated the dependence of emerging CV complications on the level of BP, the state of carbohydrate metabolism, and the blood lipid spectrum. Arterial hypertension in people with diabetes is 3 times more common than in people without diabetes and is an additional risk factor for the development of atherosclerosis and CVD [18].Numerous epidemiological studies have repeatedly demonstrated the relationship between the concentration of total cholesterol in the blood and the risk of developing CV complications, in particular acute myocardial infarction. According to studies conducted by the State Research Center for Preventive Medicine, in Russia, an increase in total cholesterol concentration of more than 194 mg/dL is observed in 65.2% of men and 62.1% of women over 30 years old. Already at a young age, the frequency of hypercholesterolemia reaches more than 41% in men and more than 51% in women, and in the group of 55–64 years, it increases to 75.7% and 82.4%, respectively [19].Attention is drawn to the fact that studied patients with CVD revealed high levels of total cholesterol, triglycerides, LDL-C and low level of HDL-C. In the group of patients included in our study, the average level of total cholesterol in the initial serum concentration was 232.06 ± 43.20 mg/dL, the initial serum triglyceride concentration was 200.85 ± 83.82 mg/dL, the initial serum LDL-C concentration was 149.20 ± 37.63 mg/dL and the initial serum HDL-C concentration was - 46.29 ± 18.03 mg/dL (p<0.005).Treatment with rosuvastatin 5 to 30 mg for a month, resulted in up to 71,75 mg/dL of LDL-C reduction (Table 6), which resulted in mean LDL-C levels of 97,7 mg/dL at the end of the study (Table 5), which is still above target LDL-C level for very high-risk patients. In reduction of CV disease, each mg/dL reduction of LDL-C is important. However, the treatment to the target LDL-C levels provide optimal CV risk reduction. The current guidelines suggest that in very high-risk patients LDL-C should be lowered to less than 54g/ml and 50% of LDL-C lowering from baseline should be achieved. The achieved average LDL-C of 97.75±22.08 is above the target level for very high-risk patients. All patients in the study had CHD, thus very high CV risk and such patients generally require the most intensive lipid-lowering therapy. Not achieving target LDL-C was due to low usage of 20 mg and 30 mg of rosuvastatin, the only two strengths that achieved reduction of LDL-C more than 50% from baseline. The latter strengths were used only in one quarter of patients. The prescribed doses of rosuvastatin were too low, resulting in undertreatment of patients, therefore higher doses of rosuvastatin should be used in most of the patients to achieve target LDL-C levels. The data are also consistent with the results of the ARGO study, which included 18273 patients also from various federal districts in Russian Federation. Hypercholesterolemia was detected in 81.3% of women and 78.9% of men. In all federal districts in Russian Federation, the level of total cholesterol in patients was significantly higher than the target and ranged from 225 mg/dL to 236 mg/dL, while statins were prescribed only to half of the patients [20].Measurement of BP, lipids and lipoproteins is used to estimate the CV risk, using SCORE (2, 2-OP) scale and guide therapeutic decision-making in the treatment of HCL. LDL-C is the primary target for the treatment strategies for HCL and reduction of CV risk, and statins are the core of lipid-lowering therapy [8]. International multicenter study PURE proved that high mortality rates from circulatory system diseases in countries with low per capita income are associated with a lack of use of major classes of drugs, including statins [21]. The availability of the statins in Uzbekistan increased with introduction of added value generic high intensity statins, which are a cornerstone lipid-lowering therapy. High burden of CVD in Uzbekistan should result prescription of high dosages of these molecules, however this is not the case.Along with patient education on prevention of CVD, we have to raise an awareness also among physicians, about the primary prevention of CVD and secondary prevention in patients with already established CVD, with focus on detecting high BP and lipid levels on regular basis. Lowering BP with guidelines endorsed SPC to target levels and reduction of LDL-C to target levels with high-intensity statin as recommended in guidelines, especially in high and very high-risk patients, could help in flattening the curve of high CVD mortality in Uzbekistan.
Conflicts of Interest
- No potential conflicts of interest.
Funding
- This article research work was funded personally by the author.