Shamsiev Jamshed Azamatovich, Khurramov Firdavs Abdusmatovich
Specialized Pediatric Surgical Clinic of SamSMU, Samarkand, Uzbekistan
Correspondence to: Khurramov Firdavs Abdusmatovich, Specialized Pediatric Surgical Clinic of SamSMU, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
This article presents the results of traditional and minimally invasive methods of treatment of acute spermatic cord cyst in 355 children. Acute spermatic cord cyst (ASCC) in children, it is one of the frequent and at the same time poorly studied pathologies. Despite the abundance of literary sources devoted to diseases associated with impaired obliteration of the vaginal process, there are very few studies on ASCC. There is no single approach to the management of patients with this pathology.
Keywords:
Spermatic cord cyst, Puncture, Control group, Main group, Acute
Cite this paper: Shamsiev Jamshed Azamatovich, Khurramov Firdavs Abdusmatovich, For the Treatment of Acute Spermatic Cord Cyst in Children, American Journal of Medicine and Medical Sciences, Vol. 13 No. 12, 2023, pp. 2062-2065. doi: 10.5923/j.ajmms.20231312.52.
1. Introduction
There is no consensus among pediatric surgeons regarding the treatment tactics for ASCC in children. There are adherents of radical treatment tactics, at the same time there are many specialists who prefer the puncture method of treatment. Adherents of radical correction explain their choice by the fact that the operation allows you to get rid of the disease once and for all. However, at the same time there are no exact recommendations on how to deal with patients who have contraindications to the anesthetic manual.Proponents of the puncture method of treatment of ASCC explain their choice by the fact that surgical intervention is advisable only if the results of the puncture method are unsatisfactory. The choice of this tactic is justified by the properties of the vaginal process of the peritoneum in young children to obliteration. At the same time, the possibility of repeated punctures is allowed. At the same time, being a minimally invasive puncture method of treatment of ASCC is considered as the most attractive. With the right tactical approach, the availability of hardware visual monitoring in real time and the safest possible methods of ASCC puncture, this method, with a number of advantages, can be a full-fledged alternative to the surgical method.
2. Material and Methods
In the specialized pediatric surgical clinic of the Samarkand State Medical University for the period from 1994 to 2021, 355 patients with ASCC under the age of 1 year were treated. Depending on the treatment tactics, the patients were divided into 2 groups. The control group consisted of 160 (45.1%) patients whose treatment did not adhere to certain treatment tactics. Patients with CG received both puncture and surgical treatment. The main group (MG) included 195 (54.9%) children. In this group, the developed treatment tactics were used, which determines the method of treatment of ASCC depending on the age of the patient.Of 355 patients, right-sided cyst location was noted in 224 (63.1%) cases, left-sided location in 125 (35.2%) and bilateral cysts were diagnosed in 6 (1.7%) patients. The sizes of cysts ranged from 2.0 cm to 3.5-4.0 cm. in diameter. Both groups were dominated by children under the age of 3 months. In CG (n=160) there were 127 (79.4%), in MG (n=195) patients under the age of 3 masses there were 149 (76.4%).
3. Results and Discussion
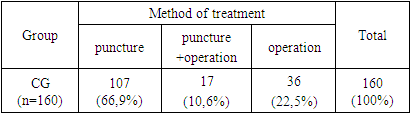
Until 2007, there was no clearly defined treatment tactics in our clinic, with ASAC. The therapeutic tactic was that we tried to adhere to a gentle method of treatment – puncture of the cyst and evacuation of its contents. The puncture was also performed in cases where there were contraindications to the anesthetic aid due to concomitant colds. With tense cysts, with their large sizes, as well as with the ineffectiveness of punctures, radical surgery was performed.Table 1. Methods of treatment of ASCC in CG
 |
| |
|
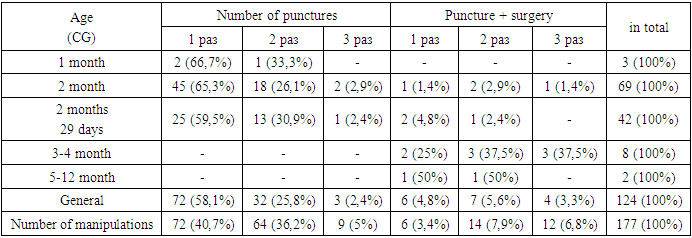
Table 1 shows that out of 160 CG children, 107 (66.9%) were treated with a puncture method, 17 (10.6%) due to the lack of effect from punctures, surgical excision of the cyst was performed as planned. A total of 124 (77.5%) children were punctured. The reason for the use of puncture treatment was the presence of medical contraindications to the anesthetic aid in patients (see Table 1). Parents of 93 (58.1%) children refused surgical treatment.It can be seen from Table 1 that 36 (22.5%) patients were operated on shortly after admission, they did not use the puncture method of treatment of ASCC. Of these, 22 (13.8%) children were operated on urgently. The indication for emergency intervention was the diagnosis – "strangulated hernia". 19 (11.9%) patients were admitted to the clinic from family polyclinics with a diagnosis of a strangulated hernia, and 3 (1.9%) patients received this diagnosis in the clinic (it was not possible to exclude a strangulated hernia). In these patients, the diagnosis of ASCC was established intraoperatively.ASCC puncture in KG was carried out using a disposable syringe with a needle, in compliance with all the requirements of asepsis and antiseptics, under local anesthesia. The puncture technique consisted in piercing the cyst wall with a conventional disposable needle at an angle of 450, the direction of the needle from the root of the scrotum towards the cyst. After entering the cavity, the liquid contents were evacuated using a syringe. The usefulness of cyst emptying was controlled by palpation, i.e. subjectively. The anxiety and mobility of the child during the puncture created difficulties when fixing the needle in a stationary state. Given the presence of sharpened edges of a disposable metal needle, any accidental movement of the latter, especially at the end of the manipulation, when the cyst subsides, can lead to damage to blood vessels or soft tissues. The specified technical features of performing an ASCC puncture in CG required certain skills from the surgeon.Table 2. The multiplicity of ASCC puncture in CG
 |
| |
|
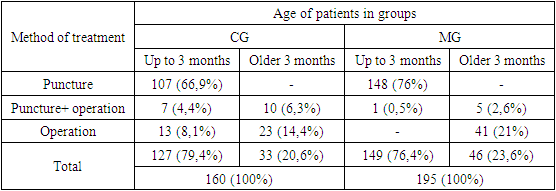
Table 2 shows that the puncture method of treatment was effective in children under the age of 3 months (2 months 29 days). Thus, in children under the age of 1 month, the effectiveness of puncture treatment was 100%, while only 1 (33.3%) puncture was performed twice. In patients aged 1 to 2 months, puncture treatment was achieved in 65 (94.2%), and in 39 (92.9%) aged 2 to 3 months. In patients from 3 months and older, even repeated punctures were not effective.Analysis of the results of puncture treatment of ASCC showed that this method of treatment was highly effective in patients under the age of 3 months. Thus, the effectiveness of the puncture method of treatment of ASCC, which was applied to 114 children under the age of 3 months, was effective in 107 (93.9%) cases. In 10 patients aged 3 months and older, the puncture method of treatment was ineffective.Analysis of the results of puncture treatment of ASCC showed that this method of treatment was highly effective in patients under the age of 3 months. Thus, the effectiveness of the puncture method of treatment of ASCC, which was applied to 114 children under the age of 3 months, was effective in 107 (93.9%) cases. In 10 patients aged 3 months and older, the puncture method of treatment was ineffective.At the same time, the method of puncture of ASCC in CG needed modernization. The use of a standard, disposable, injection needle with cutting edges during puncture of ASCC in CG led to complications such as damage to blood vessels, through-piercing of the cyst. The lack of hardware visual control forced the surgeon to rely only on palpatory sensations. This could not give reliable information about the complete emptying of the cyst. The reliability of palpation decreased even more with repeated punctures, due to swelling of soft tissues and contraction of the cyst walls.For the puncture treatment of ASCC in patients with MG, a method has been proposed that is characterized by minimal trauma to soft tissues, eliminating damage to blood vessels during aspiration of the liquid contents of the cyst. Minimal traumatization of soft tissues during puncture was achieved by using a disposable angiocatheter, which has thin, elastic walls and is equipped with a needle with a special laser sharpening, which provides an atraumatic and painless introduction. Full-fledged, high-quality emptying of the cyst was monitored by ultrasound examination in real time.The methods of treatment of ASCC in the compared groups are shown in Table 3. For the convenience of comparative analysis, the data in the groups are given separately for children under 3 months and older than 3 months. As can be seen from Table 3, 107 (66.9%) children under 3 months of age in KG were cured by traditional puncture, 7 (4.4%) patients at this age underwent surgery after ineffective puncture, and 13 (8.1%) due to the difficulty of differential diagnosis with a strangulated hernia, lack of methodology ultrasound diagnostics of ASCC immediately performed the operation. In contrast to CG in MG, 148 (76.0%) children under the age of 3 months had a gentle method of puncture treatment of ASCC. In 1 (0.5%) case, due to the refusal of the parents, the second puncture was not performed on the child, and at the insistence of the parents, surgical excision of the cyst was performed. It should be noted that 5 children in the MG, whose age was older than 3 months, were punctured before surgical excision of the cyst. In these 5 cases, the puncture was performed as a palliative method, because the children had temporary contraindications to general anesthesia. It can be concluded that 13 CG children under the age of 3 months (is 8.1% in relation to the total number of CG patients or 10.2% in relation to children under the age of 3 months of this group) ASCC could be cured by the puncture method and thereby avoid "vain" surgical intervention. As can be seen from Table 3 in the MG for children under 3 months, "wasted" operations decreased from 10.2% to 0.5%.Table 3. Methods of treatment of ASCC in the compared groups
 |
| |
|
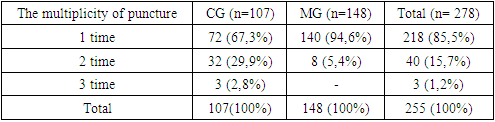
To achieve a therapeutic effect, in some cases, repeated punctures were performed for children with ASCC. To determine the effectiveness of the developed gentle method of puncture treatment of ASCC, we compared the multiplicity of punctures in both study groups. The multiplicity of punctures in the compared groups performed to obtain a therapeutic effect is shown in Table 4.Table 4. The multiplicity of punctures in the compared groups performed on patients who recovered only from the puncture method of treatment
 |
| |
|
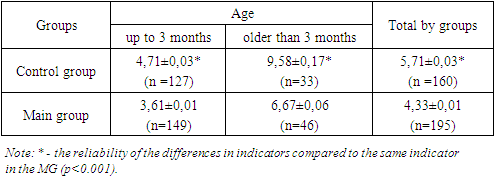
Table 4 shows that in KG, the number of patients who recovered only from the puncture method was 107 children, and in MG - 148. The data given in Table 4 show that in CG, to achieve a therapeutic effect, 32 (29.9%) patients underwent double punctures, and 3 (2.8%) punctures completed 3 times. As a result of the use of a new gentle method of puncture treatment, the effectiveness of a single puncture increased from 67.3% in CG to 94.6% in MG. The number of patients who underwent double puncture decreased from 29.9% in CG to 5.4% in MG. The number of patients with triple puncture decreased from 2.8% in CG to 0% in MG. Simple calculations show that in order to improve the health of children in CG, 107 children underwent 145 punctures by the traditional method, i.e. in a ratio of 1:1.35. In MG, 148 children underwent a total of 156 punctures by the new gentle method (ratio 1:1.04). In conclusion of the analysis of Table 4, it should be noted that the number of punctures necessary for the recovery of children from ASCC in the MG was reduced by 1.3 times, i.e. by 30.0%, compared with CG.The proposed method of treatment of ASCC made it possible to significantly reduce the length of stay of patients in the hospital (Table 5).Table 5. The length of stay of patients in the hospital in the compared groups
 |
| |
|
The data given in Table 5 show that the use of the proposed method of treatment of ASCC allowed to significantly reduce (p<0.001) the length of stay of patients under the age of 3 months from 4.71±0.03 in CG to 3.61±0.01 in MG, among children over the age of 3 months to significantly reduce (p<0.001) from 9.58±0.17 in CG to 6.67±0.06 in exhaust. There is also a significant (p<0.001) reduction in the length of stay in the hospital of patients with MG in general compared with CG (4.33±0.01 and 5.71±0.03, respectively).
4. Conclusions
1. The conducted studies have shown the dependence of the results of the puncture method of treatment of ASCC on age. The older the patient's age, the less effective the puncture method of treatment.2. Analysis of the results of treatment of patients in G showed that the puncture method of treatment of ASCC is more effective in children under the age of 3 months.3. The proposed gentle method of differentiated treatment of ASCC allowed to increase the number of effective punctures in the MG by 10%, reduce ineffective punctures by 3 times (from 10.6% in CG to 3.1% in MG), reduce surgical intervention from 12.5% to 0.5%, reduce bed days from 5.71± 0.03 to 4.33±0.01 (p<0.001).
References
| [1] | Shamsiev Zh.A., F.A. Khurramov, I.A. Mutalibov / Minimally invasive method of treatment of acute spermatic cord cyst in children // Proceedings of the 4th International Scientific and Practical Conference "Science and Practice: Implementation to Modern Society" (May 6-8, 2020). Manchester, Great Britain. - pp.387-390. |
| [2] | Shamsiev Zh.A., F.A. Khurramov, D.O. Atakulov. / Histomorphological structure of an acute spermatic cord cyst in newborns and young children // International independent scientific journal. - 2020, - No.34, - pp.42-45. Aydemir H. / Inflammatory myofibroblastic tumor of the spermatic cord: two cases and review of the literature // Ann Saudi Med. - 2020 Jan-Feb. - 40(1). - Р.66-71. |
| [3] | Shamsiev J.A., Shamsiev A.M., Khurramov F.A., Suvonkulov U.T./ Tactics of treatment of acute funiculocele in children // A New Day in Medicine (No. 10.2023) Uzbekistan pp. 245-248. |
| [4] | Shchedrov D.N. Medvedev N.A. "Acute diseases of the scrotum organs in newborns". "Bulletin of Urology" 2014, No. 4., pp. 25-35. |
| [5] | Babikov. V.M. "Surgical correction of impaired obliteration of the vaginal process of the peritoneum in children". / V.M. Babikov // Surgery of childhood. -2013. -№2 (39). - Pp. 25-29. |
| [6] | Chang YT, Lee JY, Wang JY, Chiou CS, Chang CC. Hydrocele of the spermatic cord in infants and children: its particular characteristics. Urology. 2010 Jul; 76(1): 82-6. |
| [7] | Rhodes HL, Corbett HJ, Horwood JF, Losty PD. Neonatal testicular torsion: a survey of current practice amongst paediatric surgeons and urologists in the United Kingdom and Ireland. J Pediatr Surg. 2011 Nov; 46(11): 2157-60. |
| [8] | Pritula V.P., Povoroznyuk V.S., Maksakova I.S., Rybalchenko I.G. Syndrome of edematous and enlarged scrotum in newborns and young children: issues of diagnosis and treatment. // Surgery of childhood. 2015. No. 1-2 (46-47). pp. 88-94. |
| [9] | Reznichenko A.G., Dolgikh O.Yu., Amosov A.V., Demidko Yu.L. Surgical treatment of funiculocele and hydrocele after inguinal hernioplasty // Questions of urology and andrology. 2018. Vol. 6. No. 1. pp. 31-34. |
| [10] | Tarakanov V.A. and co-authors " Inguinal hernias in children. Dropsy of the testicular membranes. Cryptorchidism. Educational and methodical manual. Krasnodar 2011. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML