-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2023; 13(12): 1993-1996
doi:10.5923/j.ajmms.20231312.37
Received: Nov. 23, 2023; Accepted: Dec. 10, 2023; Published: Dec. 23, 2023

Antenatal Ultrasonographic Diagnosis of Congenital Partial Intestinal Obstruction
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLJ. B. Sattarov, A. V. Ibragimov
Tashkent Pediatric Medical Institute, Republican Educational and Methodological Center for Neonatal Surgery at the Republican Perinatal Center, Tashkent, Uzbekistan
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: In this study, we explored the utility of ultrasound imaging in diagnosing and managing developmental anomalies of the intestinal tract in fetuses and newborns. Focusing on cases of intestinal obstruction, we investigated the diagnostic accuracy and prognostic value of ultrasound in predicting postoperative complications. Methods: A comprehensive analysis was conducted on a cohort of pregnant women and their newborns presenting with suspected intestinal anomalies. Ultrasound examinations were performed during various stages of pregnancy and postnatally to assess the presence, type, and severity of intestinal obstructions. The study involved a detailed examination of echoscopic features, including identifying the vermiform appendix, signs of acute or chronic obstruction, and abnormal positioning of internal organs. Results: Ultrasound demonstrated a high diagnostic accuracy in identifying and characterizing developmental anomalies of the intestinal tract. The technique proved particularly effective in diagnosing low forms of intestinal obstruction. Additionally, specific ultrasound signs, such as a heterogeneous intestine with dilation of intestinal loops, were identified as prognostically unfavorable, aiding in predicting postoperative outcomes. Conclusion: Our findings highlight the significance of ultrasound as a valuable tool in the antenatal and postnatal diagnosis of intestinal anomalies. The information gathered from ultrasound examinations facilitated informed decision-making regarding pregnancy management, delivery strategies, and postoperative care for newborns with identified pathologies.
Keywords: Congenital intestinal obstruction, Ultrasound diagnosis, Children
Cite this paper: J. B. Sattarov, A. V. Ibragimov, Antenatal Ultrasonographic Diagnosis of Congenital Partial Intestinal Obstruction, American Journal of Medicine and Medical Sciences, Vol. 13 No. 12, 2023, pp. 1993-1996. doi: 10.5923/j.ajmms.20231312.37.
1. Introduction
- The birth of children with developmental anomalies poses a significant and not only medical but also social problem. This pathology remains one of the severe complications of pregnancy and ranks first among the causes of childhood disability and mortality [3]. Many authors [1,6,7,12] note that against the backdrop of decreasing fertility, the frequency of fetal developmental anomalies is increasing without a trend of reducing the birth of children with developmental defects [3,6,8]. Therefore, it is crucial to detect deviations in fetal development as early as possible and provide prospective parents with complete information about their child's development prospects. In this regard, prenatal diagnosis becomes particularly important as it enables the identification of various developmental defects in the early stages of pregnancy and facilitates decision-making regarding the further management of pregnancy. Despite the widespread use of ultrasound examination (US), prenatal diagnosis of congenital disabilities leaves much to be desired [3,9,15].The most common pathology in neonatal surgery is congenital intestinal obstruction (CIO), which is recorded with a frequency of 1:2000 newborns. However, prognostic criteria for the course of intestinal obstruction leading to local and systemic complications still need to be developed [4,5,13]. The prospective use of transabdominal ultrasound examination of the intestines is considered a non-invasive and highly informative method, allowing for obtaining information about the condition rapidly and, importantly, painlessly for the newborn [2,9,11].The echoscopic semiotics of acquired intestinal obstruction is more extensively represented in the literature, while data on ultrasonic diagnosis of congenital partial intestinal obstruction (CPIO) are scarce and dedicated to ultrasonic diagnosis of CPIO as a variant of CIO in newborns and infants, describing individual cases or based on a limited clinical material [5,10].Among the diagnostic methods for congenital developmental defects, including CIO, antenatal ultrasound diagnosis (USD) of pregnant women is the primary method. The advantages of USD lie in the non-invasiveness and reliability of information on the development and condition of almost all organs and systems of the fetus. The task of prenatal diagnosis is not only to establish the fact of a congenital defect in the gastrointestinal tract but also to identify associated anomalies and chromosomal aberrations. Despite the widespread use of ultrasound, prenatal diagnosis of gastrointestinal developmental defects poses significant challenges.This study aims to improve the diagnosis of CPIO based on antenatal ultrasound diagnosis, summarize our observations, and analyze literature data on the significance of ultrasound studies in comprehensive diagnostics.
2. Materials and Methods
- From 2015 to 2022, at various gestational ages, ultrasound examinations were conducted on 50,790 pregnant women at the Perinatal Center of the Ministry of Health of the Republic of Uzbekistan. During the same period, 45,580 deliveries were registered at the center: 45,127 (99.0%) live births and 453 (0.99%) stillbirths. The diagnosis of congenital intestinal obstruction was established in 463 (1.0%) cases. Ultrasound examinations were performed using real-time devices: "Siemens S 60 S" (Germany), "Logiq E 9," "Voluson E 8 expert" (USA) - with the use of transabdominal and transvaginal probes with frequencies of 3.5; 7.5 MHz.
3. Results and Discussion
- In cases where surgical pathology of the abdominal organs was suspected, the examination of 123 patients began with ultrasonic visualization of the abdominal organs. In 53 (43.1%) of them, signs of intestinal obstruction were detected or suspected during antenatal examination. The examination was carried out to promptly confirm or exclude a previously established diagnosis and identify developmental defects and diseases not diagnosed by previous examinations or arising due to complicated intra- and postnatal periods. For this purpose, echocardiography and neurosonography were included in the study's complex. The obtained data were taken into account when determining the compatibility or incompatibility of the identified pathologies with the child's life, the timing of surgical intervention, and preventive, diagnostic, and therapeutic measures in the early neonatal period. Special attention was paid to identifying the main and indirect signs of intestinal obstruction: fluid deposition in the intestinal lumen, differences in the diameter of the intestines, thickness, and uniformity of the wall, peristalsis characteristics in different segments; the extent, localization of the dilatation and narrowing of the intestine, the presence of interintestinal adhesions, the mobility of intestinal loops, the detection of the vermiform appendix with clarification of its location; the accumulation of effusion in the abdominal cavity. The data analysis allows for an assessment of the nature of intestinal obstruction (complete or partial) and its localization (high, low) and determines the plan for further investigations. Congenital intestinal obstruction is characterized by an acute course in the neonatal period or a chronic recurrent course in infants. Severe complications of intestinal obstruction include ischemia and subsequent necrosis with the development of peritonitis. Impaired mesenteric blood circulation in the basin of the upper mesenteric vessels is the most common manifestation of intestinal rotation defects, often with a recurrent course.According to certain authors, congenital intestinal obstruction (CIO) can be detected prenatally, even in the first trimester of pregnancy, and in the second half of pregnancy, the diagnosis is generally not challenging [9-12]. The literature presents characteristic ultrasound images of various clinical-anatomical forms of CIO in fetuses and newborns. The identification of congenital torsion during malrotation of the fetal intestine indicates the prospectiveness of antenatal diagnosis of gastrointestinal developmental defects. Using ultrasound, conditions such as cystic fibrosis, peritonitis, and reverse positioning of internal organs in combination with intestinal obstruction (seen in multiple organ malrotation syndrome) can be identified. Based on literature data and our own observations, we provide a typical echo signature for congenital intestinal obstruction in fetuses, valuable for radiologists, pediatric surgeons, and neonatologists.In the study of obstetric-gynecological history, deviations from the physiological course of pregnancy were noted in 87 (70.7%) mothers of affected children, with factors provoking dysfunction and anomalies in the development of the gastrointestinal tract organs. The development of various types and severity of pathology required conservative therapy with negative consequences.Chronic fetal hypoxia negatively influences the formation of the child's organs and systems during critical periods of intrauterine development. Complicated pregnancies pose a high risk of abnormal deliveries, particularly fetal hypoxia.Out of 123 children, low birth weight (2500 g or less) was observed in 15 (12.2%). With a large weight (4000 g or more), there were 8 (7.3%) newborns.From the history of 123 women who gave birth to children with developmental defects, menstrual cycle irregularities were found in 11 (8.9%), inflammatory processes of the female reproductive organs in 29 (23.6%), chlamydia in 3 (2.4%), chronic pyelonephritis in 15 (12.2%), a combination of several disorders in 33 (26.8%). Artificial abortions occurred in 5 (4.1%), spontaneous abortions before 12 weeks in 7 (5.7%); at 16-18 weeks in 4 (3.3%); missed pregnancies in 3 (2.4%); full-term births in 99 (80.5%); preterm births in 15 (12.2%); late births in 9 (7.3%). In 63 (51.2%) of the 123 patients, this pregnancy was complicated by anemia, threatening miscarriage in the early stages in 39 (31.7%), threatening early preterm births at 32-34 weeks in 6 (4.9%); exacerbation of chronic pyelonephritis in 15 (12.2%).Out of the 123 women, 92 (74.8%) delivered vaginally, and 8 (25.2%) underwent cesarean section.Indications for surgery: pelvic presentation, clinically narrow pelvis, weak labor activity, acute fetal hypoxia. All 123 women gave birth to children with developmental anomalies.Out of 29 (23.6%) newborns, 20 (69.0%) had associated anomalies in addition to the main defect: congenital heart defects - 7, genitourinary system anomalies - 3, central nervous system developmental defects - 5, gastrointestinal tract defects - 3, musculoskeletal system defects - 2. Nine children had more than 2 associated defects. Multiple developmental defects were found in 9 newborns (31.0%); among those with high intestinal obstruction, congenital heart defects and Down syndrome were more frequently observed.Antenatal ultrasound (US) reveals indirect echographic signs of the intraintestinal membrane. This membrane, covering the intestinal lumen, results from the impaired expansion of the inner layer of the duodenum (Figure 1). The intestinal lumen is narrowed by several millimeters, and the contours of the mucous membrane are clear. This pathology does not warrant pregnancy termination. Malrotation involves the disruption of the normal rotation and fixation of the duodenum. Full rotation of the midgut on its blood supply stalk can lead to the cessation of its blood supply and subsequent necrosis. On ultrasound, an anechoic double-bubble is identified due to the expansion of the intestine and stomach. Even minor dilation at 16-22 weeks should cause concern. Normally, the duodenum is visible on ultrasound only from the 24th week. Stenosis is a partial obstruction of the duodenum, localized in one place. It is mainly observed in the upper parts and is accompanied by anomalies of the pancreas. It is clearly visible during Doppler examination of intestinal blood flow. Stenosis can be successfully eliminated and has more favorable prospects than atresia. It does not require pregnancy termination. Megaduodenum is an enlargement of the duodenum exceeding the size of the stomach. It can result from a ring-shaped pancreas, where the head of the organ encircles the intestine, or from atresia or stenosis of the duodenum. It is diagnosed on ultrasound at 24 weeks. The upper part of the abdominal cavity is significantly distended, and the lower part is concave.
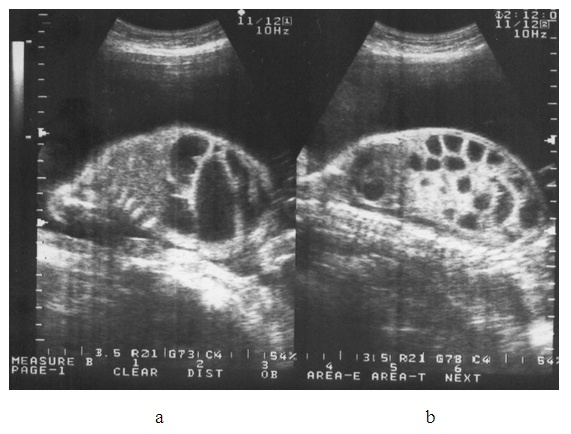 | Figure 1. a) Sonogram of high intestinal obstruction in a fetus of a 29-year-old pregnant woman (Patient F) at 32 weeks of gestation, showing the presence of a double-bubble sign. b) Sonogram of low intestinal obstruction in a fetus of a 21-year-old pregnant woman (Patient A) at 28 weeks of gestation, revealing multiple anechoic fluid-filled formations |
4. Conclusions
- In the majority of cases, ultrasound imaging enables accurate diagnosis of developmental anomalies of the intestinal tract and aids in selecting a rational approach to pregnancy management, mode of delivery, optimal timing, and method of treatment for newborns considering the identified pathology.Ultrasound examination in the diagnosis of intestinal obstruction in newborns holds high diagnostic and prognostic value, allowing for the prediction of postoperative complications within the abdominal cavity. Before surgery, sonography demonstrates higher accuracy in diagnosing low forms of intestinal obstruction compared to high forms. A prognostically unfavorable ultrasound sign is the combination of a heterogeneous intestine with dilation of intestinal loops.During abdominal ultrasound imaging, special attention should be paid to the absence of the vermiform appendix or its identification in atypical locations, echoscopic signs of acute or chronic intestinal obstruction, and abnormal positioning of internal organs, indicating the risk of malrotation.