-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2023; 13(12): 1847-1850
doi:10.5923/j.ajmms.20231312.05
Received: Nov. 1, 2023; Accepted: Nov. 26, 2023; Published: Dec. 2, 2023

Preoperative Diagnosis of Patients with Nodular Goiter
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSalokhiddinov Jurabek Saidakhmadovich
Samarkand State Medical University, Samarkand, Republic of Uzbekistan
Correspondence to: Salokhiddinov Jurabek Saidakhmadovich, Samarkand State Medical University, Samarkand, Republic of Uzbekistan.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The study included the results of an examination of 112 patients with toxic forms of goiter. Methods for complex preoperative diagnosis of toxic forms of goiter should include ultrasound and CT, which make it possible to non-invasively obtain information about the size, topography, echostructure of the thyroid gland and pathological formations detected in it, as well as to study the condition of the zones of regional lymphatic drainage. Radionuclide scanning is indicated for autonomous thyroid nodules, relapse of toxic goiter, and atypical localization of the thyroid gland. A hormonal study of thyroid function includes determining the concentration of TTH, T3, T4, thyroid binding globulin and the titer of antibodies to thyroglobulin.
Keywords: Toxic goiter, Research methods
Cite this paper: Salokhiddinov Jurabek Saidakhmadovich, Preoperative Diagnosis of Patients with Nodular Goiter, American Journal of Medicine and Medical Sciences, Vol. 13 No. 12, 2023, pp. 1847-1850. doi: 10.5923/j.ajmms.20231312.05.
Article Outline
1. Introduction
- According to the World Health Organization, "more than 750 million people worldwide are affected by thyroid pathology, while patients with diffuse and mixed toxic goiter occupy the first place among thyroid diseases." Due to the lack of a downward trend in the number of patients and the existence of endemic regions, where the incidence rate varies from 1.2 to 9.0 per 100,000 population, thyroid diseases continue to be a serious medical and social problem, including in Uzbekistan, despite the long-term struggle with iodine deficiency.At the present stage, the diagnosis of toxic goiter forms does not present significant difficulties, largely due to the emergence of non-invasive imaging methods, the information content of which reaches 95-100% in a complex application. At the same time, the lack of alertness leads to late diagnosis and, consequently, an increase in complicated forms of the disease.
2. Purpose of the Study
- Optimization of diagnostic methods for toxic forms of thyroid diseases.
3. Material and Methods of Research
- The study is based on the results of examination of 112 patients with toxic goiter forms who were admitted to the surgical departments of the multidisciplinary clinic of Samarkand State Medical University and City Clinical Hospital No. 1 in the period from 2012 to 2021.Female patients prevailed – 88 (78.6%), men – 24 (21.4%). The patients ranged in age from 21 to 65 years.Out of 112 patients, 102 (91.1%) patients were diagnosed with toxic goiter for the first time, 10 (8.9%) patients had recurrent toxic goiter, of which 8 patients had primary relapse. Out of 10 patients, 6 patients underwent the first operation in our clinic in different years. 4 had a history of strumectomy in other hospitals. Postoperative recurrent goiter was detected up to 5 years in 7 patients and up to 10 years in 3. It should be noted that among 10 patients with recurrent toxic goiter, 3 patients had primary multi-node non-toxic goiter basedified within 3 years, the remaining 7 patients were operated earlier for diffuse toxic goiter.The size of the degree of thyroid enlargement in patients with toxic goiter forms was evaluated according to the classification of O. V. Nikolaev based on ultrasound and palpation of the thyroid gland, and 43 (38.4%) patients were diagnosed with a toxic goiter form of II-III degree, 69 (61.6%) IV-V degree.The severity of thyrotoxicosis was assessed on the basis of physical criteria according to the classification of V. G. Baranov: mild was detected in 35 (31.2%), moderate in 52 (46.4%) and severe in 25 (22.3%) patients.Pathomorphologically, diffuse toxic goiter was detected in 50 (44.6%) patients, mixed toxic goiter in 39 (34.8%), toxic adenoma in 13 (11.6%) and recurrent toxic goiter in 10 (8.9%) patients.Before being referred for surgery, patients were observed for a long time and received conservative therapy. Up to 1 year of treatment, 7 (6.2%) patients were treated, 29 (25.9%) patients were treated from 1 year to 3 years, and 76 (67.8%) patients were treated for more than 3 years.
4. Research Results and Discussion
- All patients with toxic forms of goiter were examined according to a single comprehensive scheme, which included interviewing and examining the patient, taking blood for laboratory analysis and conducting an instrumental study.When interviewing patients, they specified their profession, the nature of work and place of residence, their complaints, the time of their appearance, and the presence of thyroid diseases in relatives.During the examination, attention was paid to the size and deformity of the neck (its configuration), the condition of the eyeballs, the presence or absence of finger tremor, and the condition of the skin (dryness, humidity, puffiness, pigmentation).The presence of a nodular formation that shifts when swallowing in the projection of the thyroid gland of one or another density in the absence of cytological signs of neoplastic growth allowed us to think of a nodular goiter. At the same time, the presence of multiple formations in the thyroid gland, signs of infiltration of tissues on the neck indicated thyroid cancer, which required a thorough differential diagnosis.Anamnesis collection and physical examination revealed ophthalmopathy, thyroid dysfunction, and the degree of its enlargement.Most often, patients with toxic forms of goiter complained of neck pain (44.6%), limb tremor (63.4%), palpitation (56.2%), increased blood pressure (64.3%), weight loss (48.2%), and changes in the eyes.The severity of the condition of patients with thyroid pathology was largely determined by concomitant diseases.Coronary heart disease (22.3%), hypertension (20.5%), and diabetes mellitus (4.5%) significantly affected the prognosis of the disease course. Among patients with toxic goiter who received antithyroid therapy, a high percentage of cholelithiasis (25.0%), peptic ulcer of the stomach and duodenum (16.9%), chronic pancreatitis (13.4%), and chronic diseases of the large intestine (14.3%) were noted. Ultrasound examination of the thyroid gland and areas of regional lymph outflow was performed in real time, i.e. at baseline and at different times after surgery (Fig. 1).
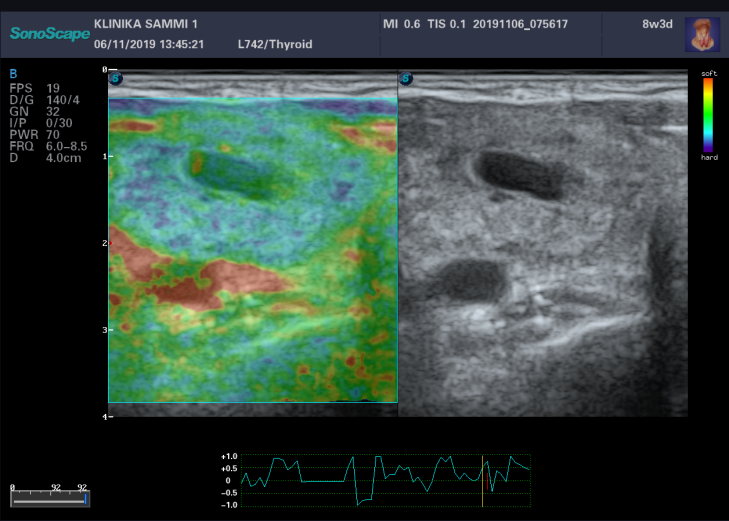 | Figure 1. Thyroid ultrasound. In the left thyroid lobe, a nodular formation with a volume of up to 20 cm3 is determined |
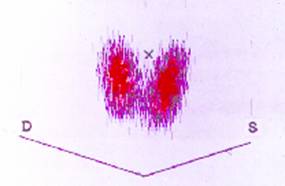 | Figure 2. Thyroid scan. Diffuse toxic goiter |
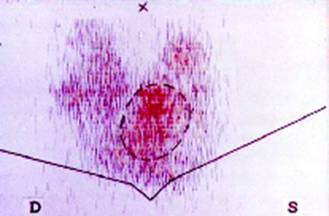 | Figure 3. Thyroid scan. "Hot knot" in the left thyroid lobe. Toxic adenoma |
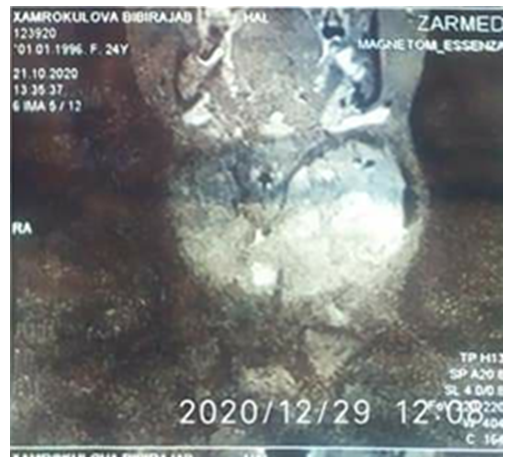
 | Figure 4. Thyroid CT scan. Multi-node goiter |
 | Figure 5. Thyroid CT scan. Toxic IV grade IV adenoma |
5. Conclusions
- 1. Methods of preoperative diagnosis of toxic goiter forms should include ultrasound and CT, which allow noninvasively obtaining information about the size, topography, and echostructure of the thyroid gland and the pathological formations detected in it, as well as studying the state of regional lymph outflow zones.2. Radionuclide scanning is indicated for autonomous thyroid nodules, recurrent toxic goiter, and atypical thyroid localization.3. Hormonal tests of thyroid function include determination of TSH,T3,T4, thyroid-binding globulin and anti-thyroglobulin antibody titer. An increase in TSH levels suggested hypothyroidism, while a decrease in TSH levels suggested thyrotoxicosis. An increase in T3 and T4 concentrations4 confirmed the presence of thyrotoxicosis.Information about the source of support in the form of grants, equipment, and drugs. The authors did not receive financial support from manufacturers of medicines and medical equipment.Conflicts of interest: The authors have no conflicts of interest.