-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2023; 13(11): 1805-1807
doi:10.5923/j.ajmms.20231311.43
Received: Oct. 22, 2023; Accepted: Nov. 20, 2023; Published: Nov. 25, 2023

Features of Management of Children with Congenal Cataracts and Accompanying Visual Pathology
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbdurakhmanova Charos , Buzrukov Batir , Makhmudova Dilorom , Abdullaeva Durdona
Tashkent Pediatric Medical Institute, Tashkent, Uzbekistan
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

An analysis of the case histories of 72 children (117 eyes) diagnosed with congenital cataracts, who were hospitalized in the eye department of the TashPMI clinic for the period from 2016 to 2023 at the age of 3 months to 14 years, was carried out. The study revealed that, children with congenital cataracts and concomitant pathology of the visual organ require a differentiated approach to patient management: in the presence of microphthalmos, early surgical intervention is necessary before 1 year - stage 1, including cataract extraction, followed by stage 2 - IOL implantation. Constant dynamic monitoring is necessary, given the high percentage of postoperative complications.
Keywords: Congenital cataract, Concomitant pathology, Microphthalmia, IOL implantation
Cite this paper: Abdurakhmanova Charos , Buzrukov Batir , Makhmudova Dilorom , Abdullaeva Durdona , Features of Management of Children with Congenal Cataracts and Accompanying Visual Pathology, American Journal of Medicine and Medical Sciences, Vol. 13 No. 11, 2023, pp. 1805-1807. doi: 10.5923/j.ajmms.20231311.43.
Article Outline
1. Introduction
- One of the common causes of blindness and low vision in children is congenital pathology of the lens, namely cataracts, which account for up to 10-19.5% [5,7,9,16]. Congenital cataracts (CC) are observed in 5 cases out of 100,000 newborns and cause 10-38% of cases of childhood blindness [5]. Cataract is a persistent clouding of the substance of the lens or its bag, accompanied by a decrease in visual acuity from a slight weakening to light perception. Congenital cataracts are often combined with other pathological changes in the organ of vision, which are observed in 36.8-77.3% of children: strabismus, nystagmus, microphthalmos, microcornea and other anomalies of the cornea, as well as the vitreous body, choroid, retina and optic nerve. Strabismus is observed in 30.2-83.3% of children with congenital cataracts. More often it is converging, alternating, predominantly constant. Nystagmus is observed in 14.0-58.8% of children with congenital cataracts; it can be congenital or acquired, associated with a sharp decrease in vision. More often it is pendulum-shaped, horizontal, less often - jerky. Microphthalmos is a congenital anomaly that is often associated with congenital cataracts in 22.5% of cases due to its characteristic structures including a thickened sclera, a normal or slightly larger lens with a relatively small eye volume, a higher lens-to-eye volume ratio, and a shallow anterior chamber, narrow camera angle and short ocular axis. Microphthalmos can cause glaucoma and other complications affecting the retina and choroid. Congenital cataract with complex microphthalmos is often combined with ocular or systemic abnormalities, and patients after surgery are prone to secondary glaucoma, corneal opacification and other serious complications [10,11,14,15]. Depending on the size of the eye, there are 3 degrees of microphthalmos: 1 degree - a decrease in one or two of the above dimensions by 1.0-1.5 mm compared to the age norm; 2nd degree - decrease by 2.0-2.5 mm; 3rd degree - reduction by 3mm or more. Features of congenital cataracts with microphthalmia are predominantly complete opacities of the lens - 66.7% (zonular are 2.7%), a high percentage of capsulo-lenticular opacities - 67.1%, a narrow rigid pupil and its various anomalies, even absence. The most common change in the cornea in congenital cataracts is a change in its size - microcornea. Colobomas of the iris are often encountered, which vary widely in size and shape and are often located in the lower segment [4]. Severe anomalies are various manifestations of mesodermal dysgenesis. Cataract is one of the elements of Rieger's syndrome (dysgenesis of the iris and cornea) and Peters syndrome (mesodermal-ectodermal dysgenesis of the cornea and iris). CC is also part of the Persistent hyperplastic primary vitreous (PHPV). PHPV is associated with a disruption of the process of regression of the primary embryonic vitreous body. Changes in the retina and optic nerve of varying nature and severity, identified in 55% of cases, are one of the reasons for low visual acuity after extraction of congenital cataracts. More often, combined lesions were observed (40.5%), less often - isolated changes in the retina (5.0%) or optic nerve (9.5%). Pathologies of the optic nerve included partial atrophy and developmental abnormalities (reduction in size, change in disc shape, etc.). On the part of the retina, macular hypoplasia, myelin fibers, central and peripheral dystrophy, “old” chorioretinal lesions (multiple, small, in the periphery, or large in the central region) were detected [2,3]. Treatment of congenital cataracts in children remains a serious problem, which is associated not only with the anatomical features of the structure of the child’s eye, but also with the frequency of concomitant pathologies, as well as with various complications caused by the hyperergic state of the child’s immune system [7,6,8,16].One of the most important questions remains about the timing of surgical intervention for congenital cataracts. Currently, most authors are of the opinion that complete, layered and central cataracts with an opacification area of more than 2.5 mm should be operated on within the first three months after the birth of the child [1,3], and for para central and central cataracts less than 2.5 mm in diameter - dynamic observation is possible. Proponents of a more radical approach insist on surgical treatment of congenital cataracts after a clinical diagnosis of the disease has been established [12]. However, despite different views, in most cases the problem of early surgical intervention is solved individually in each case, taking into account not only the degree of intensity of lens opacification, but also the presence and severity of combined pathology of the visual analyzer and the child’s body as a whole [13,14].Purpose of the study. To study the features of management of children with congenital cataracts and concomitant pathologies of the visual organ.
2. Material and Research Methods
- An analysis of the case histories of 72 children (117 eyes) diagnosed with congenital cataracts, who were hospitalized in the eye department of the TashPMI clinic for the period from 2016 to 2023 at the age of 3 months to 14 years, was carried out. Boys made up 42%, girls 58%. A bilateral process is observed in 45 (62%), unilateral in 27 (38%) children. The patients underwent visometry, biomicroscopy, keratometry, ophthalmoscopy, tonometry, echobiometry, strabismus angle determination, and visual evoked potential (VEP) study. Preoperative preparation also included consultations with a pediatrician and neurologist; if necessary, children were consulted by a geneticist, an ophthalmologist, and other specialists.
3. Research Results and Discussion
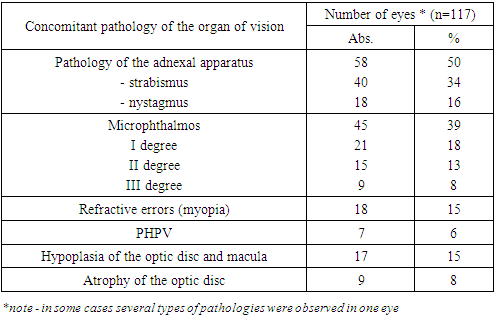
- According to the clinical and surgical classification of congenital cataracts [5], “layered” (nuclear, zonular) were observed in 22 (19%) eyes, “total” cataracts in 38 (32%), “atypical” cataracts (semi-resolved, calcified, anteroposterior capsular, posterior and anterior lenticonus) in 57 (49%) children. In patients, the range of concomitant pathologies was quite wide (Table 1).
|
4. Conclusions
- Thus, children with congenital cataracts and concomitant pathology of the visual organ require a differentiated approach to patient management: in the presence of microphthalmos, early surgical intervention is necessary before 1 year - stage 1, including cataract extraction, followed by stage 2 - IOL implantation. Constant dynamic monitoring is necessary, given the high percentage of postoperative complications. It is also necessary to carry out the following rehabilitation measures: glasses correction, measures aimed at combating amblyopia, if necessary, nootropic therapy, YAG - laser capsulotomy.