-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2023; 13(10): 1564-1568
doi:10.5923/j.ajmms.20231310.41
Received: Oct. 2, 2023; Accepted: Oct. 18, 2023; Published: Oct. 21, 2023

Prognostic Role of Immune-Inflammatory Biomarkers in Patients with Acute Ischemic Stroke
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRakhimbaeva G. S., Abdurakhmonova K. B.
Department of Neurology, Tashkent Medical Academy, Tashkent, Uzbekistan
Correspondence to: Abdurakhmonova K. B., Department of Neurology, Tashkent Medical Academy, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background. It is clear that, inflammation worsen cerebral injury at the acute phase of stroke. Immune-inflammatory processes proceed during the all periods of acute ischemic stroke and effect on outcomes of a stroke. Neutrophils, lymphocytes and platelets are main blood cells of the immune-inflammatory system and can quickly be assessed during regular laboratory studies. Objectives. The purpose of our research was to investigate the association between Neutrophil-to-lymphocyte ratio, lymphocyte-to-monocyte ratio and systemic immune-inflammation index and the prognosis of acute ischemic stroke over 3-months period. Methods. 118 patients with acute ischemic stroke who treated at Tashkent Medical Academy were included in the study. The fasting blood within 24 hours of admission was collected to determine the concentration of the clinical indicators. The functional prognosis was assessed using the modified Rankin Scale (mRS) 3 months after stroke. The poor prognosis is described as mRS ≥ 3. Predictive ability of each biomarker has also been evaluated with ROC analysis. Results. Neutrophil-to-lymphocyte ratio and systemic immune-inflammation index were found to be independent predictors of 3-month outcome (odds ratio (OR) =1.1; 95% confidence interval (95% CI), 1.064–1.134; p = 0.04) (area under the curve (AUC) =0.751%) and (odds ratio (OR) =1.0; 95% confidence interval (95% CI), 1–1; p = 0.007) (area under the curve (AUC) =0.784 %), respectively. Independent associations with functional outcome were not established for lymphocyte-to-monocyte ratio. Conclusions. Our study demonstrated that high Neutrophil-to-lymphocyte ratio and systemic immune-inflammation index at emergency department admission could be useful marker for predicting poor functional outcome at 3 months after stroke, while lymphocyte-to-monocyte ratio was not correlated with functional outcome.
Keywords: Stroke, Outcome, Systemic immune-inflammation index, Neutrophil-to-lymphocyte ratio, Lymphocyte-to-monocyte ratio, Prognosis
Cite this paper: Rakhimbaeva G. S., Abdurakhmonova K. B., Prognostic Role of Immune-Inflammatory Biomarkers in Patients with Acute Ischemic Stroke, American Journal of Medicine and Medical Sciences, Vol. 13 No. 10, 2023, pp. 1564-1568. doi: 10.5923/j.ajmms.20231310.41.
Article Outline
1. Introduction
- It is clear that, the stroke is one of the most frequent cause of the global disease burden. The death and disability percent of stroke are remarkably high, with 13.7 million new stroke events in a year, and 5.8 million morbidity due to stroke [1]. The pathological processes which are underlying of Acute Ischemic Stroke (AIS) are complicated [2]. Results of many recent studies show that, inflammation plays an crucial role in the development and occurrence of AIS [3]. Immune-inflammatory processes proceed during the all periods of AIS and effect on outcomes of a stroke [4]. Neutrophils, lymphocytes and platelets are main blood cells of the immune-inflammatory system and can quickly be assessed during regular laboratory studies [5]. Neutrophil-to-lymphocyte ratio (NLR), lymphocyte-to-monocyte ratio (LMR) and systemic immune-inflammation index (SII), which are derived from platelet, neutrophil, monocyte and lymphocyte counts, properly reflect the balance between innate and adaptive immunity [6,7]. Nowadays, hematology analyzers are fully automated and provide a complete blood count (CBC) panel, that contains 5-part differential WBCs and platelet immediately. The hematological markers of inflammation in the CBC panel are useful in predicting the outcome of the diseases. The acute stress can rise neutrophil counts but decrease the number of lymphocytes. Previous studies have showed that higher neutrophil counts before thrombolysis for AIS can cause poor outcome and degree of stroke severity [8,9]. SII, a new immune-inflammatory ratio developed by Hu et al., was established to be a powerful indicator of poor functional outcomes in patients with hepatocellular carcinoma [7]. Higher SII is correlated with worsening in cancer, endocarditis, coronary artery disease, and dementia [6,10-13]. Moreover, the lymphocyte-to- monocyte ratio (LMR) is connected to a poor outcome of hematologic and solid malignancies [14,15]. Besides that, a low LMR ratio predicts moderate to severe stroke independently and has been proved to be an independent factor for predicting poor functional outcome of stroke patients treated with thrombolysis or routine therapy [16,17].NLR and LMR are representative of the peripheral neutrophil and lymphocyte counts and the peripheral lymphocyte and monocyte counts; respectively, and SII incorporates the lymphocyte, neutrophil, and platelet counts into an index. Purpose of this study is to assess the prognostic values of NLR, PLR, and SII upon emergency department (ED) admission to predict neurological recovery in AIS over 3-months follow-up. The importance of these parameters and their association with the functional outcome have not been fully studied in patients with AIS.
2. Subjects and Methods
2.1. Study Population
- From January 2022 to June 2022, AIS patients who were treated at Tashkent Medical Academy were included in the study. After screening, a total of 118 patients were included in the study. To detemine the early stage of the immune-inflammatory process, only patients who were admitted within 4 days of symptom onset were enrolled. AIS was defined by clinical presentation and proof of an ischemic lesion or absence of a corresponding intracranial lesion other than infarction by using brain computed tomography (CT) or magnetic resonance imaging (MRI). The exclusion criteria contains stroke history, combined with tumor, combined with infectious disease or autoimmune disease, and combined with cerebral hemorrhage. The study complied with the Declaration of Helsinki and was approved by the local medical ethics committee. Research subjects or guardians agree to participate in the research and sign an informed consent form.
2.2. Characteristics of AIS Patients
- All patients underwent full neurological examination. Past medical history (hypertension, diabetes, coronary heart disease, and atrial fibrillation) and demographic data were asked and collected. An electronic sphygmomanometer is used to determine the blood pressure of patients. Outcome was determined at 3 months with modified Rankin Scale (mRS) score by a neurologist.
2.3. Blood Collection
- For each included participants, blood samples were collected within 24 hours of admission. All blood samples centrifuged within 30 minutes at low temperature and high speed. Separate and pack the serum and store it in a refrigerator at -20°C until the measuring procedure started.
2.4. The CBC, Including WBCs, Neutrophil Counts, Lymphocyte Counts, Monocyte Counts and Platelet Counts, was Determined
- The NLR, the LMR, and the SII were analyzed and calculated as follows: NLR=neutrophil counts/lymphocyte counts, LMR= lymphocyte counts/monocyte counts, and SII=platelet counts x neutrophil counts/lymphocyte counts.
2.5. Functional Outcome
- The modified Rankin Scale (mRS) was used to assess the degree of disability or dependence upon ED admission and 3 month follow-up after a stroke. The score ranged from 0 (no disability) to 6 (death), and each subsequent level indicated progressive functional impairment. A good prognosis is defined as mRS < 3, and a poor prognosis is defined as mRS ≥ 3. Patient with AIS were divided into the good outcome group and poor outcome group according to the difference of mRS scores.
2.6. Statistical Analyses
- Continuous variables were reported as mean ± standard deviation. The receiver operating characteristic curve is applied to assess the cut point of ICAM-1 and hs-CRP to differentiate between good and poor outcomes. Logistic regression analysis were used to determine the independent contribution of different variables to prognosis prediction. Statistical analysis was performed using SPSS 29.0 software (SPSS Inc., Chicago, Illinois, USA), and p value <0.05 was set statistically significant.
3. Results
3.1. Characteristics of AIS Patients
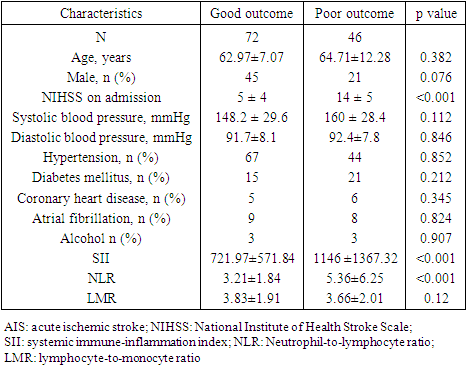
- This study included 118 AIS patients. According to the mRS score, they were divided into 2 groups, which are a good outcome group (n = 72) and a poor outcome group (n = 46). A good outcome was noticed in 61% of these patients. The population’s clinical characteristics and comparisons according to outcome are shown in the Table 1. The ages of AIS patients in the good outcome group and poor outcome group were (62.97±7.07) and (64.71±12.28) years, respectively. First group included 62.5% men with AIS, while second group consists of 45.6% men. Significant statistical difference was not determined between two groups in age and gender. We further compared the past medical history of the two groups of AIS patients, and we found that their incidence of hypertension, diabetes, coronary heart disease, alcohol consumption and atrial fibrillation was not significantly different (p > 0.05). Regarding clinical indicators, such as systolic blood pressure, diastolic blood pressure, there was also no significant statistical difference between the two groups (p > 0.05). NIHSS score at admission (p < 0.001) were remarkably higher in comparison with patient with a poor outcome. However, the average SII and NLR values were also higher in the poor outcome group in comparison with good outcome group (p<0.001). When it comes to LMR value, there was no significant statistical difference between the two groups (p = 0.12).
|
3.2. ROC Analysis for the Immune-Inflammatory Markers
- The ROC curve analysis of SII demonstrated that the area under the curve (AUC) was 0,784 and the critical threshold value was 514.56, with sensitivity of 80% and specificity of 40%, while the NLR showed that the AUC was 0.751 and the cutoff value was 2.83, sensitivity and specificity were 73.3% and 40% respectively. The ROC curve analysis of LMR showed that AUC was 0.33 which means statistical insignificant.
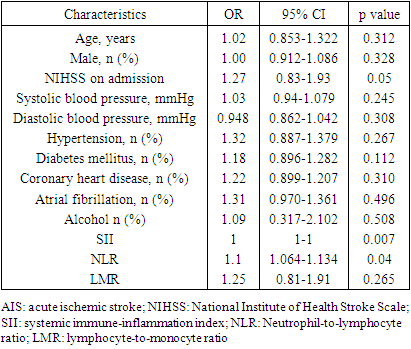
3.3. Logistic Regression Analyses
- Table 2 shows the predictive value of several clinical baseline characteristics which were incorporated into logistic regression analyses. The results of logistic regression demonstrated that after adjusting for baseline characteristics, SII and NLR ratios are still the predictors of poor outcome at 3 months in patients with AIS ((p =0.007 and p = 0.04, respectively).
|
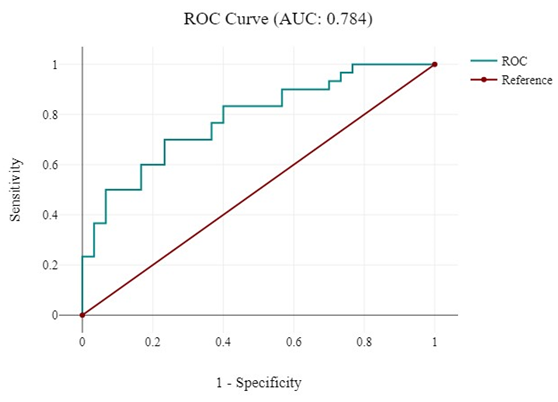 | Figure 1. ROC analyses of SII |
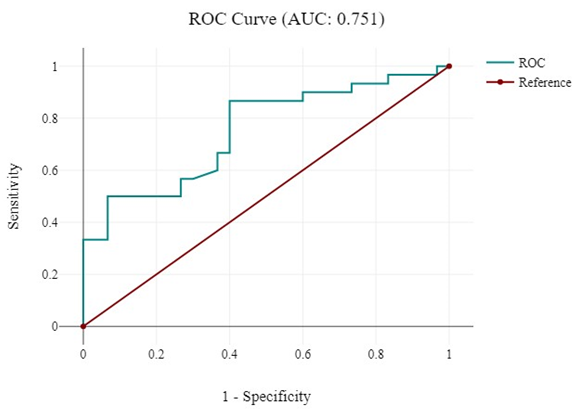 | Figure 2. ROC analyses of NLR |
4. Discussion
- Our study showed that SII and NLR values are significantly higher in patients with poor AIS outcomes than those with good outcome after 3-months period after AIS while LMR was not associated with the 3-months outcome of AIS. Innate immunity, consisting of neutrophils, monocytes, macrophages and complement systems, allows the first line of rapid attack against pathogens. Adaptive immunity, also called as acquired immunity, contains mainly lymphocytes and is the second line of protection against pathogens. Neutrophils emigrate to the injured area within 6–24 hours after cerebral ischemia, producing several cytokines and engaging in the early destruction of the blood-brain barrier (BBB) [18]. Lymphocytes gather in the brain 3–6 days after AIS, considerably later than neutrophils [19,20]. Furthermore, mediating hemostasis and thrombosis, platelets also take part in immune-inflammatory reaction by releasing mediators to increase inflammation after AIS and bring about the release of neutrophils and lymphocytes into the vessel wall [21]. Activation of microglia, macrophages, and mast cells due to cerebral ischemia results in release of proinflammatory cytokines, which in turn causes a release of stress hormones by activation of both sympathetic and hypothalamic-pituitary-adrenal axis systems [22]. Complicated immune-inflammatory reactions, the conversion of identified single blood cell counts into ratios of cell measurement, such as NLR, LMR and SII, appears to be more appropriate to the balance between innate and adaptive immunity [12,13].In this study, we found that NLR and SII ratios were higher in patients with poor outcome in comparison with good outcome group. Neutrophil level elevates several hours after symptom onset and may remain for several days. A moderate increasing of lymphocytes could be expected several days after AIS and may last for several weeks. However, the CBC parameters can easily help to predict functional outcome after AIS. In this research, 3 hematological inflammatory biomarkers with the advantage of free available in the routine blood test are evaluated. The results demonstrated that the immune-inflammatory biomarkers at admission are remarkably negatively correlated with clinical outcome improvement in patients with AIS at the first 90 days poststroke. Limitation of the study. This study had several limitations. First of all, this study was carried out using registry data and subject to the limitations of any retrospective analysis. Secondly, we only calculated NLR, LMR, and SII ratio at ED admission. Studies revealed that these biomarkers could vary after AIS. Finally, the neurological recovery hinge on care standards after stroke and rehabilitation. The patient compliance may affect the prognostic values of the several parameters for outcomes in patients with acute ischemic stroke.
5. Conclusions
- Our study demonstrated that high NLR and SII at ED admission could be useful marker for predicting poor functional outcome at 3 months after stroke, while LMR was not correlated with functional outcome. In conclusion, NLR and SII values could help clinicians to recognize and take measures for treatment in the early stage of the disease.
ACKNOWLEDGEMENTS
- We thank all individuals who agreed to participate in this study.
Funding
- This study is not supported by any organization.
Competing Interests
- All the authors declare no conflict of interests.