-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2023; 13(9): 1351-1355
doi:10.5923/j.ajmms.20231309.40
Received: Sep. 19, 2023; Accepted: Sep. 27, 2023; Published: Sep. 28, 2023

Study of the Effect of COVID-19 Infection on Thyroid Tissue State
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKarimova M. M. 1, Shamansurova Z. M. 2
1Fergana Public Health Medical Institute
2Institute of Biophysics and Biochemistry at the National University of Uzbekistan
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article under discussion evaluates the effect of COVID-19 infection on thyroid tissue in patients without and with a history of thyroid disease according to ultrasound (USG) and histology data. The results showed that in 200 individuals with no history of thyroid disease after undergoing COVID-19, the gland enlarged to degree III in 34% and degree IV in 2%. In those with a history of thyroid disease after COVID-19, multiple nodular changes in the thyroid gland were detected, and histological examination confirmed thyroid cancer in 2% of patients.
Keywords: Coronavirus infection, COVID-19, Thyroid gland, Thyroiditis
Cite this paper: Karimova M. M. , Shamansurova Z. M. , Study of the Effect of COVID-19 Infection on Thyroid Tissue State, American Journal of Medicine and Medical Sciences, Vol. 13 No. 9, 2023, pp. 1351-1355. doi: 10.5923/j.ajmms.20231309.40.
Article Outline
1. The Relevance of the Research Topic
- COVID-19 and its complications continue to be a global problem worldwide [13]. Patients with comorbidities, especially endocrine diseases, have a more severe course of this disease. Thyroid dysfunction is manifested both during the acute phase of COVID -19 infection and during the recovery period after COVID-19, as reported in some literature [8]. Many authors believe, that the thyroid dysfunction induced in COVID - 19 patients is due to the effects of a "cytokine storm" causing autoimmune diseases of the thyroid gland [17], even an exacerbation of Graves' disease has been reported [2]. In patients with thyroid diseases are already known changes in the immune system, weakening of immunity [19]. It has been proven in a number of scientific works that the Fergana Valley is a region with severe iodine deficiency [5]. Iodine deficiency will inevitably have its own features in COVID - 19 disease, especially in patients with pre-existing thyroid diseases. Scientific studies related to iodine-deficient COVID-19 infection have been insufficient worldwide, and the study of thyroid function after COVID-19 infection in people with autoimmune thyroid diseases and nodular and multinodular goitre in Fergana region, which is an iodine deficiency zone, is of great importance. It is necessary to conduct additional informational and scientific studies on this issue in order to deeply understand the influence and mechanisms of pathogenesis of COVID-19 in the acute phase and late stages of the disease on the development and late stage of thyroid diseases, as well as to develop effective recommendations for treatment and clinical control. Taking into account the above mentioned, the study of the peculiarities of the course of COVID-19 infection in patients with thyroid diseases was recognised as one of the urgent medical issues in our region, especially in Fergana region. The aim of the research: to evaluate the effect of COVID-19 infection on thyroid tissue.
2. Objects and Methods of the Research
- The data on morbidity among residents of Fergana region of 350 patients who applied to the private clinic of "Doctor Fatkhullo" LLC in 2019-2023 were analysed. Among the patients examined, 295 (84%) were female and 55(14%) were male, whose age ranged from 18 to 73 years.The patients' disease data were scrutinised to determine the duration of disease course, whether thyroid disease was diagnosed before COVID-19 infection, the patients' general clinical presentation, palpation of the thyroid gland and determination of the degree of enlargement according to WHO classification, determination of thyroid tissue status by ultrasound and evaluation of findings according to TIRADS classification, if thyroid nodules were present to conduct histological fine-needle aspiration biopsy and evaluation of it.Patients were divided into 2 groups during the period of achievement of these scores. Group 1 consisted of 200 patients with a history of thyroid disease before COVID-19 infection (200 patients, average age 39±13.6 years). Patients in this group were treated for various thyroid diseases under the supervision of an endocrinologist before COVID-19 infection. They had degree I thyroid enlargement (52 patients), degree II enlargement (42 patients), autoimmune thyroiditis (30 patients), nodular goiter (14 patients), mixed goiter disease (10 patients), hypothyroidism (8 patients), subclinical hyperthyroidism (20 patients), there were cases of diffuse toxic goiter (24 patients). Group 2 included 150 patients with COVID-19 infection who had no history of thyroid disease. Patients in this group were not under the care of an endocrinologist before COVID-19 infection. A general clinical examination of all patients was performed, including palpation of the thyroid gland, ultrasound of the regional lymph node outflow area and thyroid gland, detection of nodules in thyroid tissue according to TIRADS category, fine-needle aspiration biopsy if nodules were present and histological studies.
3. Results Obtained
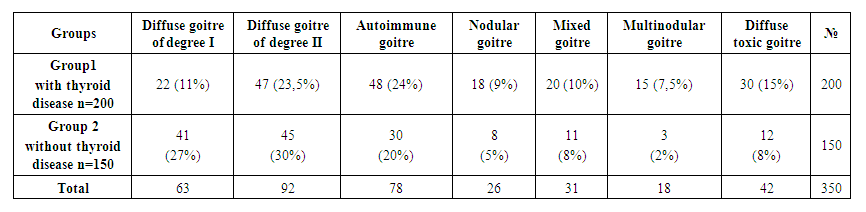
- Thyroid diseases in group 1 patients before COVID-19 infection are presented in table 1 below.
 | Table 1. Diseases detected in the thyroid prior to COVID-19 infection |
 | Table 2. Thyroid diseases after COVID - 19 infection in the examined patients |
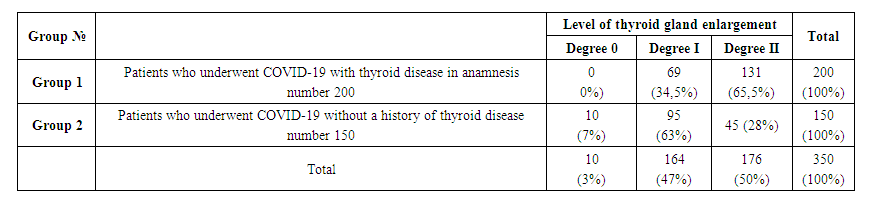 | Table 3. Degree of thyroid gland enlargement according to WHO classification in the examined patients, palpation results |
 | Table 4. Frequency of thyroid enlargement after ultrasound in the patients undergoing examination |
 | Table 5. Distribution of nodular derivations in the thyroid gland according to TIRADS category using ultrasound in the examined patients |
 | Table 6. Comparative evaluation of thyroid tissue examination using ultrasound in thyroid parenchyma after COVID-19 infection involving both groups |
4. Conclusions
- 1. It was found that individuals with no history of thyroid disease who underwent COVID-19 in Fergana region developed autoimmune thyroiditis in 10%, nodular goiter in 5%, mixed goiter in 8%, multinodular goiter in 2% and diffuse toxic goiter in 4% after COVID-19. Thyroid AIT in patients with a history of pre-existing thyroid disease was found in 19%, nodular goiter in 9%, mixed goiter in 10%, multinodular goiter in 4% and diffuse goiter in 16% of patients. 2. In those with no history of thyroid disease who underwent COVID-19 infection, nodular masses in thyroid tissue corresponded to 23% of patients in TIRADS-III category and 5% of patients in TIRADS-IV category after COVID-19. In patients with a history of thyroid disease, nodular masses in thyroid tissue corresponded to the TIRADS-III category in 26%, TIRADS-IV category in 17% and TIRADS-V category in 4% of patients. This shows that patients in this group have higher risk of malignancy. 3. COVID-19 infection tends to develop autoimmune and nodular neoplasms in the thyroid gland. However, people with pre-existing thyroid disease were found to have an increased risk of developing cancer in nodular neoplasms, and 2 patients were confirmed to have thyroid cancer.4. Patients with COVID-19 have a high risk of autoimmune and nodular malignancies in thyroid tissue during early and prolonged periods of recovery, indicating the importance of monitoring thyroid function.The fact that our studies were conducted in an area of iodine deficiency, and the literature indicates that iodine deficiency is a risk factor for thyroid cancer, suggests that COVID-19 infection causes not only autoimmunity but also accelerated cancerous processes in thyroid tissue. We believe that it is important to monitor thyroid function and tissue status during the early and long-term recovery period in people with COVID-19. Given the high risk of nodule formation and malignancy, especially in patients with a history of thyroid disease, it is important to perform COVID-19 and include it in the follow-up protocol based on the results obtained.The literature indicates that the cytokine storm that occurs during the acute period of COVID-19 infection activates autoimmune factors, causing autoimmune processes in the thyroid cell, in particular the development of autoimmune thyroiditis, Graves' disease [7]. However, in COVID-19 survivors, the activation of autoimmune processes in thyroid tissue, in particular the development of nodular goiter and even heel cancer, indicates that the infection may be caused by cell growth factors [11].