-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2023; 13(9): 1332-1335
doi:10.5923/j.ajmms.20231309.34
Received: Aug. 16, 2023; Accepted: Sep. 12, 2023; Published: Sep. 28, 2023

Assessment of the Quality of Life in Children after Surgical Treatment of Hirshprung Disease
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMamajanov Umidjon Shokirovich, Mirzakarimov Bakhromjon Halimjonovich
Department of Pediatric Surgery, Andijan State Medical Institute, Andijan, Uzbekistan
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article presents the results of studying the quality of life and functional activity of children with Hirschsprung's disease who underwent surgical treatment according to the classical Soave-Lenyushkin method and the improved De La Torre-Ortega method. The quality of life of children undergoing surgical treatment was assessed using the adapted PedsQL™4.0 scale; consisting of 21 questions assessing physical, emotional, social and role functions. An analysis of the quality of life of children with Hirschsprung's disease revealed a significant increase in indicators on all scales when using the improved technique of the De La Torre-Ortega operation up to 84.1-92.3% in relation to the group of healthy children with a change in the total score from 52.8±10.0 to 70.4±6.4 (t=6.79; p<0.001).
Keywords: Hirschsprung's disease, Quality of life, Functional activity, Children
Cite this paper: Mamajanov Umidjon Shokirovich, Mirzakarimov Bakhromjon Halimjonovich, Assessment of the Quality of Life in Children after Surgical Treatment of Hirshprung Disease, American Journal of Medicine and Medical Sciences, Vol. 13 No. 9, 2023, pp. 1332-1335. doi: 10.5923/j.ajmms.20231309.34.
Article Outline
1. Topicality
- Hirschsprung's disease (HD) is a fairly common disease. It must be stated that the incidence of Hirschsprung's disease according to T.J. Bradnock [1], has fluctuated between 1:30,000 and 1:2,000 to the total number of newborns for several decades now. According to average estimates, the incidence of Hirschsprung's disease worldwide is approximately 1 case per 5000 live births. In the vast majority of cases, the symptoms of this pathology appear already in the neonatal period or in early infancy [1]. The most optimal treatment for HD is early radical intervention with resection of the aganglionic zone.Today, in the treatment of Hirschsprung's disease, radical one-stage surgical treatment using minimally invasive surgical methods is becoming more common. Modern methods of surgical treatment of Hirschsprung's disease in newborns and young children help to improve outcomes and reduce mortality.Currently, transanal resection is one of the most commonly used treatments for HD worldwide. This method has undergone some technical changes over the past decades. However, as before, these methods are associated with many potential complications, which are often the cause of irreversible deterioration in the functional outcome and tangible social restrictions [8]. The most popular are transanal methods Soave and Swenson [7]. The introduction of these methods of surgical intervention has reduced the duration of hospitalization and reduced the number of postoperative complications. However, even with their most effective and successful application, there is a risk of developing various complications [2].In 1998, De la Torre, using simultaneous transanal endorectal resection of the large intestine for the surgical treatment of Hirschsprung's disease, leveled the use of laparotomy [3]. However, the use of this method of surgical intervention in total and subtotal forms of Hirschsprung's disease is not possible.Recently, laparoscopic surgery for HD has become the most widespread. However, as with traditional methods of treatment, this type of surgical intervention also has the following negative factors: the likelihood of postoperative complications in the form of constipation (7.1-22.2%) and infection (8.9-14.8%) [6].In recent years, the quality of life of patients with various diseases, the effectiveness of their treatment and rehabilitation have been studied [4]. When evaluating the results of surgical treatment of Hirschsprung's disease, the study of one of the aspects of the quality of life, the vital sign, is of key importance.
2. Purpose of the Research
- To study the indicators of functional activity and quality of life in children with Hirschsprung's disease operated on by the De La Torre-Ortega method.
3. Materials and Research Methods
- The study included 21 children who underwent surgery for Hirschsprung's disease in the clinics of the Department of Pediatric Surgery of Andijan State Medical Institute. The age of the patients ranged from 2 to 18 years. 4 (19.04%) patients were admitted to the clinic in the stage of decompensation, 12 (57.14%) - in the stage of subcompensation, 5 (23.8%) - in the stage of compensation. 13 (61.9%) children were operated on using the improved De La Torre-Ortega and 8 (38.1%) patients underwent transanal resection of the large intestine according to the classical Soave-Lenyushkin technique.In the course of studying the quality of life, the children with Hirschsprung's disease and their parents filled out children's and parental forms of the PedsQL™4.0 questionnaire, translated into Uzbek, before surgery and later 1 year after surgery [4,5]. The study included children from the age of two (the minimum age for assessing the quality of life). Given the small number of respondents, the results of the survey of children of different ages were summarized, respectively, the answers of parents were also generalized. Healthy children in the amount of 15 people were subjected to the survey for comparative evaluation.The questionnaire consisted of 21 questions and is represented by the following scales:- physical functioning (PF) - 8 questions,- emotional functioning (EF) - 5 questions,- social functioning (SF) - 5 questions,- role functioning (RF) - functioning in kindergarten (FK) or school functioning (SF) - 3 questions (based on the age of children).1. Physical functioning (PF), reflecting the degree to which the physical condition limits the performance of physical activities (walking, carrying heavy loads, climbing stairs, self-service, etc.).2. Emotional functioning (Role-Emotional functioning - RE) involves assessing the degree to which the emotional state interferes with the performance of work or other daily activities (including spending more time, reducing the volume of work, reducing its quality).3. Social functioning (SF) is determined by the degree to which the physical or emotional state limits social activity (communication).4. Role-Physical Functioning (RPF) - the impact of physical condition on daily role-playing activities (work, daily duties). The questionnaire has sections for age groups: 5-7, 8-12 and 13-18 years old, with forms for children and parents to fill in, and a section for children of 2-4 years old (filled in only by parents). The parents and children were asked to choose one of the proposed answers to each question in the appropriate (child and parent) form of the questionnaire. The parents of children under 5 years of age answered the questions instead of them, from 5 years of age - the children answered by themselves. The total number of points for all modules is calculated on a 100-point scale after the scaling procedure: the higher the final value, the better the child's quality of life.The statistical significance of the obtained measurements when comparing the average values was determined by the Student t-test (t) criterion with the calculation of the error probability (P) when checking the normality of the distribution (by the kurtosis criterion) and the equality of general variances (F - Fisher's criterion). The confidence level P<0.05 was taken as statistically significant changes.
4. Results of the Study and Their Discussion
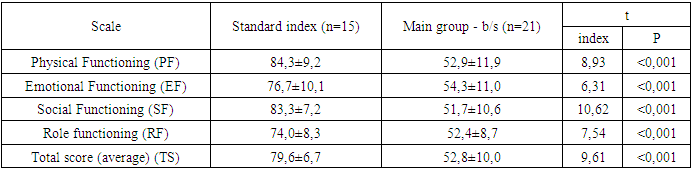
- When comparing the quality of life indicators in the group of healthy children and in the main group before surgery (Table 1), the total score (TS) in the main group before surgery (b/s) was 52.8±10.0 (t=9.61, p<0.001), while in healthy children this indicator varied within 79.6±6.7.
|
|
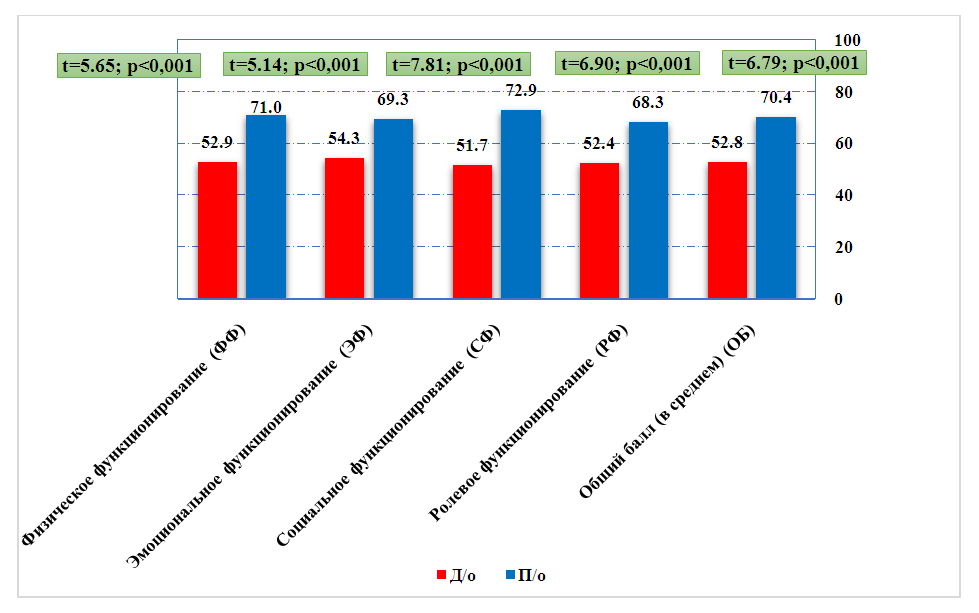 | Figure 1. Dynamics of the quality of life index in the main group before and in 12 months after surgery |
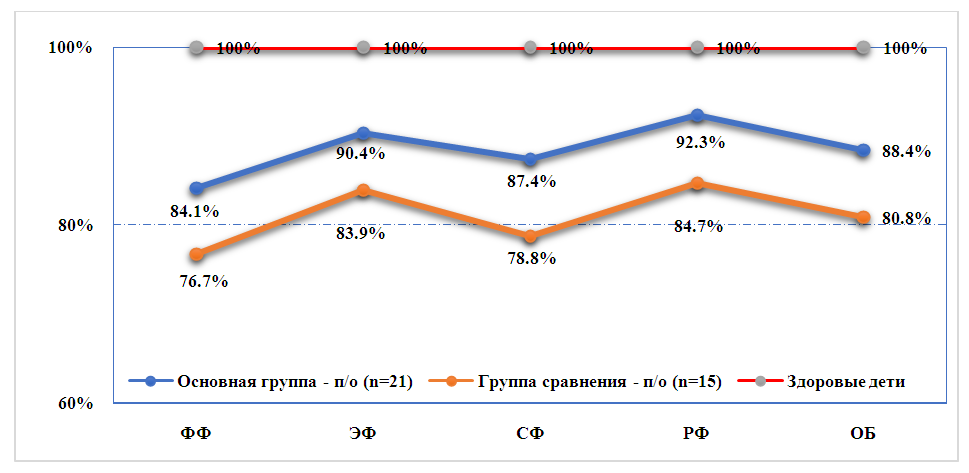 | Figure 2. The ratio of quality of life indicators in the comparison groups in 12 months after surgery to healthy children |
5. Conclusions
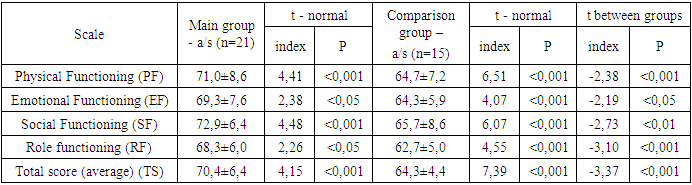
- 1. During the observation period up to 12 months after surgical treatment of children with Hirschsprung's disease in the main group, the frequency of functional and organic complications decreased (constipation, encopresis, anal canal stenosis) from 40.4% to 18.4% (χ2=4.792; Df =1; P=0.029), which generally helped increase the proportion of good results from 46.8% to 73.7% (χ2=7.046; Df=2; P=0.030).2. During the analysis of the quality of life of children with Hirschsprung's disease, a significant increase in indicators on all scales was revealed a year after surgical treatment, while the degree of improvement was higher (p<0.05) when using the improved technique of the De La Torre-Ortega operation (on average from 62.0-70.8% on all scales before surgery to 84.1-92.3% in relation to the group of healthy children) with a change in the total score from 52.8±10.0 to 70.4±6, 4 (t=6.79; p<0.001), along with this, transanal resection of the large intestine according to the classical method of Soave-Lenyushkin made it possible to achieve compliance with the group of healthy children at an average level of 76.7-84.7% with increase in the total points only up to 64.3±4.4.