Saidmurod Murtazaev, Mukhayyo Kuchkarova
Tashkent State Dental Institute, Makhtumkuli 103, Tashkent, Uzbekistan
Correspondence to: Saidmurod Murtazaev, Tashkent State Dental Institute, Makhtumkuli 103, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The frontal-vertical cephalometric proportions of the face were determined according to “Grummons” in 95 cases (55 men and 40 women) selected from Uzbek population which aged between 18 to 30 years olds with orthognathic type of occlusion. The ratio of the anterior-posterior and vertical orientation of the face proposed by the authors were used as a percentage during evaluating indicators of frontal-vertical face proportion in representatives of the Uzbek population. These indicators are used to determine the cause of anomalies in the front-to-vertical face ratio, i.e., in which part of the face there are problems, diagnosis and treatment.
Keywords:
Frontal cephalogram, Frontal-vertical ratio, “Grummons” analysis, Normal bite
Cite this paper: Saidmurod Murtazaev, Mukhayyo Kuchkarova, Cephalometric Indicators of Frontal-Vertical Ratios by “Grummons” in Representatives of Uzbek Population, American Journal of Medicine and Medical Sciences, Vol. 13 No. 9, 2023, pp. 1294-1299. doi: 10.5923/j.ajmms.20231309.25.
1. Introduction
Nowadays, scientists have obtained significant achievements in the field of orthodontics. Frontal X-Ray, including frontal cephalometry, and research on this subject cause changes and increases in opinion. Orthodontists in most cases conduct research in the sagittal direction and use lateral cephalometry in their practice. However, lateral cephalometry does not allow determining indicators of transversal anomalies. Lateral cephalometry cannot provide us with sufficient information in the diagnosis and treatment planning of anomalies of the maxillofacial region in the transversal direction. Only frontal cephalometry can help us to determine the dimensions of the upper and lower jaws in the transversal direction. Parameters, which are needed to determine the result of the expansion of the upper jaw, is one of the tormenting thing for orthodontists. Later, in the maxillofacial region, it was found that it was possible to determine not only the dimensions of the upper and lower jaws in the transversal direction, but also the dimensions of the pyriform opening of the middle part of the nose. The presence of a large amount of information obtained using these indicators showed the importance of frontal cephalometry for clinicians working in the field of orthodontics, orthopedics and orthognathic surgery [4,5]. In the process of assessing the frontal aesthetics which is facial symmetry, as the authors showed in their research, symmetry of the smile line is extremely significant not only to the upper and lower jaws, teeth and lips, but also to the nasal bones and respiratory organs. It has been proven that the middle zone of the face is associated with the respiratory system and the state of the lower jaw [6,7].If surgical intervention is necessary in case of asymmetry of the lower jaw and skull, if there are indications for the preservation of periodontal tissues of the teeth of the upper jaw, and also if it is necessary to carry out therapeutic measures only for the bones of the upper and lower jaws, world scientists have shown how important frontal cephalometry is and these studies reduce the likelihood recurrence during surgery [10,11].Thus, based on the foregoing, necessity of widely using frontal cephalometry is more emphasized in the practice of orthodontists in order to eliminate anomalies by transversal direction. Anterior cephalogram helps to make a correct diagnosis and prevent complications, especially in adolescents with crossbite.Aim of the researchThe purpose of the study is to clarify indicators of the “frontal-vertical ratio” of head and face bones on the frontal cephalogram by Grummons in representatives of the Uzbek population with orthognathic type of occlusion.
2. Materials and Methods
The study was conducted on 95 (55 men and 40 women) cases from Uzbek population with orthognathic type of occlusion. All subjects were determined by the proportion of the frontal and vertical direction of the head and facial bones in the frontal cephalogram according to “Grummons”.Analysis of Frontal Vertical ProportionsAccording to Grummons, the frontal-vertical ratios of the bones of the head and facial bones are proportional to the vertically drawn lines, and proposed the formula:Max.R: ANS-A1/ANS –Me=39,1%TotalMax.R: ANS-A1/Cg-Me=21,77%Mand.R.: B1-Me/ANS-Me=47,8%Total Mand.R.: B1-Me/Cg-Me=26,6%Max-Mand.R.: ANS-A1/B1-Me=81,8%The titles of the points and lines of the frontal cephalogram for determining the indicators of the frontal-vertical ratio are shown in figure 1. | Figure 1. Frontal-vertical ratios of points: 1-Cg - cockscomb of the ethmoid bone; 2-ANS (Anterior Nasal Spine) - the most protruding point of the nasal bone; 3-A1 - the middle between the upper central incisors at the level of the cutting edges; 4-B1 - the middle between the lower central incisors at the level of the cutting edges; 5-Me - chin center (Menton) |
The line connecting the points Cg, ANS, A1, B1 and Me, and passing through the midline of the face, forming the calculated MSR, is a line that crosses vertically the X-ray image of the face in the frontal projection. The author proved that the parameters of the face in the same frontal projection are proportional to the vertical indicators [1,8,14]. To do this, draw a transverse line from the points Cg, ANS, A1, B1 and Me on the vertical line MSR and measure the intermediate distances.In order to determine this proportion, the author has indicated the proportional relationship between the above surfaces and points as follows, and this is also shown in Figure-2.- Upper facial ratio - Cg ANS/Cg Me- Lower facial ratio - ANS Me/CgMe- Maxillary ratio - ANS-A1/ANS Me- Total maxillary ratio - ANS-A1/CgMe- Mandibular ratio - B1-Me/ANS-Me- Total mandibular ratio - B1 Me/Cg Me- Maxillo-mandibular ratio - ANS A1/B1 Me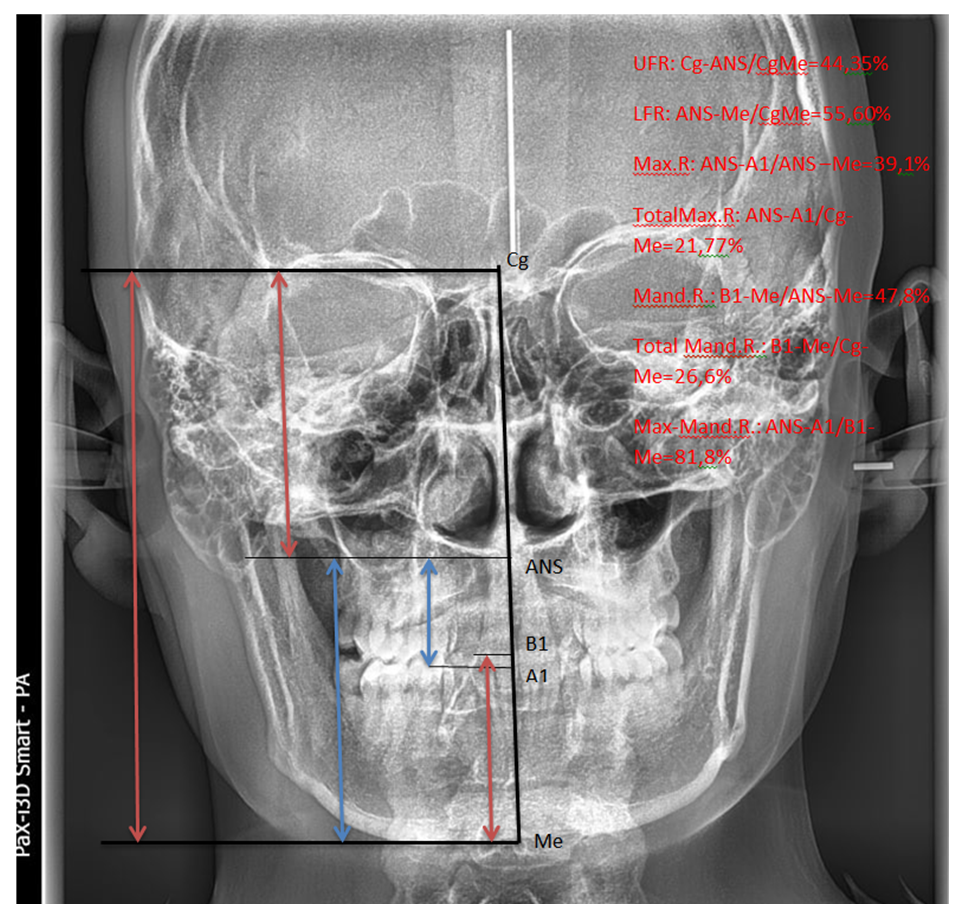 | Figure 2. Front-vertical (aesthetic) proportion. (Frontal Vertical Proportions) |
The above surfaces (lines) used in determining the indicators of the frontal vertical proportion, the author proposed to determine in percentage [1,4,13]. The main meaning of the frontal-vertical ratios is that it shows that the bones of the head-face-jaw are proportional to each other in the transversal and vertical directions (Fig. 2).- Upper facial ratio – UFR-44.35%- Lower facial ratio – LFR-55.6%- Maxillary ratio – MR-39.1%- Total maxillary ratio – Tmax R-21.77%- Mandibular ratio – Mand R-47.8%- Total mandibular ratio – Tman R-26.6%- Maxilla mandibular ratio – Mx/Mand-81.8%.
3. Results and Discussion
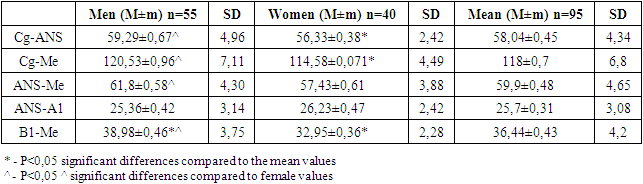
In determining these relationships, we made a computed version of the formulas in Excel-2010. We cannot compare the data of the ethnic group we are studying with the normal values of another compared ethnic group. Because when we calculate this proportion, it is recognized that each patient is selected individually. As a note, it should be noted that for the ratio of the vertical and transversal (frontal) directions, we determined and entered into the table only the distances between - Cg-ANS, Cg-Me, ANS-A1, ANS-Me, B1-Me (Table 1) [6,7,10].Table 1. Indicators used to determine the frontal-vertical ratio of representatives of the Uzbek population (mm)
 |
| |
|
In Table 1, there are presented results of gender comparison of the indicators, which were used to modify frontal-vertical ratio of the representatives of Uzbek population. The Cg-ANS index in men was 59.29±0.67 mm, in women 56.33±0.38 mm. When comparing these indicators, significant differences were found (P<0.05). As can be seen from the table, the average Cg-Me in men is 120.53±0.96 mm, and in women it is 114.58±0.071 mm. When comparing them, it was found that there is a significant difference in the Cg-Me index in men compared to the Cg-Me index in women (P<0.05).Table 1 shows that the ANS-Me index in men is 61.8±0.58 mm, in women it is 57.43±0.61 mm. When comparing the ANS-Me scores in men and women, it was found that there is a significant difference between the ANS-Me score in men and the ANS-Me score in women (P<0.05). The ANS-A1 index in men was 25.36±0.42 mm, the ANS-Me index in women was 26.23±0.47 mm. When comparing the ANS-A1 indicators of men and women of the Uzbek population, no significant differences were found (P>0.05).The B1-Me index in men averaged 38.98±0.46 mm and in women - 32.95±0.36 mm. When comparing the B1-Me indicators of men and women, it was found that a significant difference was found between the B1-Me indicator of men and the B1-Me indicator of women as well (P<0.05).The percentage values of the frontal-vertical ratio, determined in the representatives of the Uzbek population – women and men, were determined and presented in the form of a diagram (diagram 1).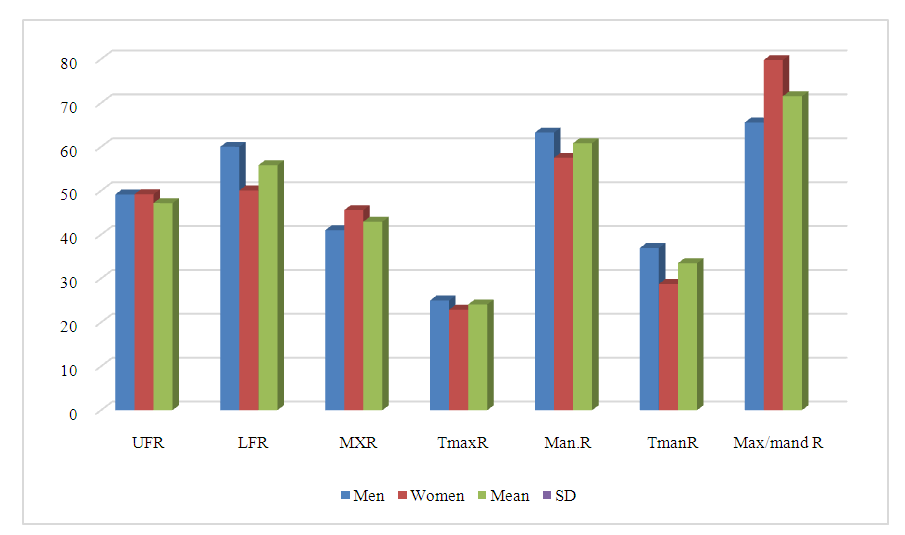 | Diagram 1. The results of indicators of the frontal-vertical ratio of representatives of the Uzbek population (in %) |
We studied the percentage indicators of the frontal-vertical ratio of the representatives of the Uzbek population in Diagram 1, and if we consider each of them, then the UFR indicator was 49.2±0.32% in women and 49.17±0.35% in men. No significant difference was found between these indicators. It was found that the LFR is 50.08±0.38% in women and 60.0±0.37% in men, and when comparing them, it was found that the difference is 10.08%. The MXR indicator was 45.59±0.52% in women and 41.00±0.51% in men, when comparing this MXR indicator, we see that the MXR indicator in women is 4.59% higher than that in men. The TmaxR index is 22.88±0.38% in women and 25.00±4.05% in men. When comparing them, it can be seen that the ratio in the middle is not so large, but is 3.22%. It was found that in the Uzbek population, the Man.R indicator is 57.51±0.60% for women and 63.26±0.86% for men, and when they are compared, a difference of 5.65% is found. The TmanR index in women is 28.76±0.27%, and in men the TmanR index is 36.95±4.51%. The diagram shows that the difference between them is 8.19%.It was established that the Max/mand R indicator in women of the Uzbek population is 79.78±1.48%, in men the Max/mand R indicator is 65.55±1.29%, and when comparing them, the found differences are 14.23% and this is shown in Diagram 1.Comparison of the obtained results with the indicators of “Grummons”To evaluate the results of the frontal-vertical ratio of the representatives of the Uzbek population, we used the indicators of the frontal-vertical ratio proposed by the author. Working on the indicators of the frontal cephalogram during his research, Grummons proposed the ratio of the frontal-vertical ratio in percent [1,4,8,9,14]. In this section, we compare the results of determining the frontal-vertical ratio in the representatives of the Uzbek population with similar indicators proposed by the author.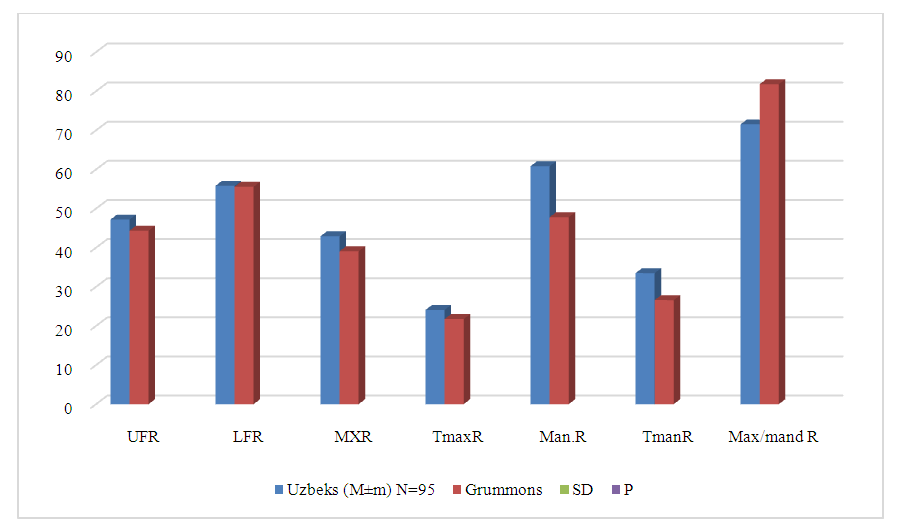 | Diagram 2. Comparison results of frontal-vertical ratio indicators of the representatives of the Uzbek population with the indicators of “Grummons” (in %) |
The frontal-vertical ratio of UFR was 47.18% in the representatives of the Uzbek population, and according to the author, it is 44.35%. The difference between them was 2.73%. In representatives of the Uzbek population, the LFR indicator is 55.82%, and it can be seen that there is no difference with the data proposed by the author in the LFR indicator -55.6% in terms of LFR. In the Uzbek population, the MXR is 42.93%, and the author's article indicates that the MXR is 39.1%, making the difference between them 2.83%. The TmaxR indicator in the representatives of the Uzbek population was equal to 24.1%, and compared with the author's TmaxR indicator (21.77%), a difference of 2.23% was revealed. The Man.R indicator of representatives of the Uzbek population is 60.84%. The author suggested that this Man.R figure is 47.8%. If we compare the indicator of the Uzbek population Man.R with the same indicator of the author, we can see that the difference is 13.04%.The author suggested that the TmanR indicator is 26.6%, the TmanR indicator of the representatives of the Uzbek population turned out to be 33.5%. When comparing them, it turned out that the difference is 6.9%.At the suggestion of the author, the Max/mand R was 81.8%. In the course of our study, we found that the Max / mand R indicator for representatives of the Uzbek population is 71.57%. Now, when we compare the Max / mand R indicators with each other, that is, the author’s Max / mand R indicator and the Uzbeks’ Max / mand R indicator, we see that the Max / mand R indicator of the representatives of the Uzbek population differs by 10.23% from the author’s indicator Max/mand R.
4. Conclusions
1. The Cg-Me index in women was equal to 114.58±0.071 mm, in men 120.53±0.96 mm, the comparison revealed a difference of 5.95±0.89 mm (P<0.05). Gender dependence should be taken into account when analyzing the indicators of the frontal-vertical ratio.2. When comparing the average indicators of the frontal-vertical ratio of women and men of the Uzbek population, it was found that in terms of Cg-Me in women, the difference is 3.42 mm, and in terms of B1-Me - 3.49 mm, and the difference in B1-Me in men was 2.54 mm (P<0.05). When analyzing Cg-Me and B1-Me indicators in Uzbeks, it was recommended to conduct an analysis taking into account gender.3. Compared with the indicators of the frontal-vertical ratio proposed by the author Grummons, the difference in the Man.R indicator was 13.04%, which was determined among representatives of the Uzbek population; the difference in TmanR was 6.9%, and the difference in Max/mand R was a flat 10.23%. When conducting a frontal cephalometric analysis according to Grummons, it is advisable to use the norms developed for the Uzbek population.
References
| [1] | Frontal Cephalometrics: ontalCephalometrics: Practical Applications, P actical Applications, Part I Robert M. Ricketts, DDS, MS1/Duane Grummons, DDS, MSD2WORLD JOURNAL OF ORTHODONTICS. |
| [2] | Ricketts RM. Application of the Frontal Headplate [in French]. Revue d’Orthopedie Dentofacial. Bioprogressive Symposium, Nantes, France, 1994. |
| [3] | Graber TM. Functional appliances. In: Graber TM, Vanarsdall RL Jr (eds). Orthodontics: Current Principles and Techniques (ed 3). St Louis: Mosby, 2000; 473–517. |
| [4] | Fränkel R. The Artificial Translation of the Mandible by Function Regulators. In: Cook JT (ed). Transactions of the Third International Orthodontic Congress. St Louis: Mosby, 1975. |
| [5] | Grummons D. Nonextraction emphasis: Space-gaining efficiencies, part I, World J Orthod 2001; 3: 1–14. |
| [6] | Ricketts RM. The Divine Proportion: A New Movement in Orthodontics. Proc Foundation Orthod Res 1980: 29–34. |
| [7] | Ricketts RM. The golden divider. J ClinOrthod 1981; 15: 752–759. |
| [8] | Ricketts RM. Respiratory obstructions and their relation to tongue posture. Cleft Palate Bulletin 1958; July: 4–5. |
| [9] | Grummons DC. Orthodontics for the TMJ/TMD Patient. Scottsdale: Wright and Co, 1994. |
| [10] | Grummons DC. Stabilizing the Occlusion: Finishing Procedures. In: Kraus SL (ed). TMJ Disorders Management of the Craniomandibular Complex. New York: Churchill Livingstone, 1988. |
| [11] | Ricketts RM. Cephalometric analysis and synthesis. Angle Orthod 1961; 31: 141–156. |
| [12] | Grummons DC. Maxillary asymmetry and frontal analysis. Clinical Impressions 1999; 8. |
| [13] | Vanarsdall RL Jr. Transverse dimension and long-term stability. Semin Orthod 1999:5:171–180. |
| [14] | Ricketts RM. Bioprogressive theory as an answer to orthodontic needs. Part II. Am J Orthod 1976; 70: 359–397. |
| [15] | Grummons DC. Transverse dimension—nonextraction emphasis. In: Bolender CJ, Bounour GH, Barat Y (eds). Extraction VersusNonextraction. Paris: SID, 1995; 151–170. |
| [16] | Ricketts RM. Facial and denture changes during orthodontic treatment as analyzed from the temporomandibular joint. Am J Orthod 1955; 41: 136. |
| [17] | Ricketts RM. Planning treatment on the basis of the facial pattern and an estimate of its growth. Angle Orthod 1957; 27: 14–37. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML