-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2023; 13(9): 1221-1223
doi:10.5923/j.ajmms.20231309.09
Received: Sep. 1, 2023; Accepted: Sep. 20, 2023; Published: Sep. 22, 2023

Differential Diagnostic Criteria in Patients with Vertigo
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLM. T. Nasretdinova, I. D. Narzullaev, N. N. Normirova, N. A. Normuradov
Samarkand Medical Institute Department of an Otorinolaringologiya, Uzbekistan
Correspondence to: M. T. Nasretdinova, Samarkand Medical Institute Department of an Otorinolaringologiya, Uzbekistan.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Dizziness is frequent reason of address to the neurologist. The study of principal reasons of dizziness became a research aim for patients. 75 patients appealings to the neurologist and otorhinolaryngologist in connection with complaints about dizziness of system character are inspected. The stated below clinical inspections allow to educe the most widespread reasons of system dizziness and in good time to suspect the critical for life of patient damages of central departments of vestibular analyzer.
Keywords: Differential diagnostic, Patients, Vertigo
Cite this paper: M. T. Nasretdinova, I. D. Narzullaev, N. N. Normirova, N. A. Normuradov, Differential Diagnostic Criteria in Patients with Vertigo, American Journal of Medicine and Medical Sciences, Vol. 13 No. 9, 2023, pp. 1221-1223. doi: 10.5923/j.ajmms.20231309.09.
1. Introduction
- Dizziness is a frequent complaint in patients who have applied for an outpatient appointment. Thus, the last large population study conducted in Germany showed that at least once during the life of vestibular vertigo experience 7.8% of the population, and the incidence of vestibular vertigo during the year is 5.2% [1].Systemic or vestibular dizziness is called the feeling of imaginary movement or rotation of surrounding objects or the patient himself in space [2]. This dizziness is caused by damage to the vestibular system and its numerous connections with other parts of the brain [3]. Systemic vertigo appears only in acute and asymmetric lesions of the vestibular system, such as loss of function or pathological irritation of one labyrinth, with damage to the vestibular nuclei on one side. [4,5].The number of diseases that cause dizziness of a systemic nature is large, and their diagnosis is difficult and requires a detailed analysis of the patient's complaints and history of the disease. Thorough research requires a special otoneurological examination, laboratory and instrumental examinations. Objective and subjective difficulties in diagnosing the causes of dizziness often lead to the fact that in practice patients with complaints of dizziness are often mistakenly diagnosed with "vegetative dystonia", "vascular crisis", "vertebral-basilar insufficiency", "hypertensive cerebral crisis" [4,6]. Meanwhile, major studies conducted in recent years show that the most common causes of dizziness may be quite different diseases: disorders of the peripheral vestibular analyzer (benign paroxysmal positional dizziness (PPDB), Meniere's disease, vestibular neuronitis) or vestibular migraine, while cerebrovascular disorders, while remaining an extremely important cause of dizziness, are relatively rare [7,8]. The aim of the study is to use diagnostic methods in patients with systemic vertigo.
2. Materials and Methods
- All patients who applied in 2018-2021 for an outpatient appointment to an otorhinolaryngologist and neurologist in the 1-Clinic SamMU were examined with complaints of dizziness. During the study period, 75 patients were contacted. The average age of patients was 49.8 ± 13.2 years. Among patients with systemic vertigo there were 52 (70.4%) women and 23 (29.6%) men (the ratio of women and men was 2: 4).Dizziness was the main and in many cases the only complaint of patients. The criteria for exclusion from the study were expressed cognitive impairment (dementia), mental disorders, severe and uncorrectable visual disorders, expressed speech disorders in the form of aphasia.When collecting anamnesis registered sex, age, profession of the patient, bad habits (Smoking, alcohol or drugs), the presence of comorbidities, drugs, specified hereditary history. The patient's use of hearing glasses, walking sticks or other to reduce the risk of falls during instability and balance disorders was recorded. Standard somatic and neurological examination was carried out. Special attention in the study of somatic status was paid to the state of the cardiovascular system (blood pressure, heart rate, the presence of edema, shortness of breath during exercise and other signs of heart failure were determined; if orthostatic hypotension was suspected, an orthostatic test was conducted).Patients underwent specific tests to assess the state of the vestibular system: the Dix—Hallpike and McClure—Pagnini positional tests, the Halmagi test, the head shake test, the Fukuda test, the Valsalva test and the hyperventilation test. In addition, the study of spontaneous, installation and positional nystagmus, visual saccades, smooth tracking eye movements, optokinetic nystagmus, caloric nystagmus was performed with the help of Frenzel glasses.Positional tests were conducted to diagnose PPDB or Central positional vertigo. A positive Dix-Hallpike test indicates canalolithiasis of the posterior semicircular canal. In a much rarer variant of DPPG with damage to the anterior semicircular canal, the Dix-Hallpike test will also be positive, but the positional torsion nystagmus will have a vertical, downward-pointing component. A McClure-Pagnini test was performed to identify the second most common variant of PPDB, horizontal semicircular channel canalithiasis. The test was considered positive if dizziness and horizontal nystagmus (geotropic or apogeotropic) occur when the head is turned in one direction or another.The appearance of atypical nystagmus during positional tests (for example, vertical, undamped, arising without a latent period, etc.) makes one suspect the so-called Central positional dizziness, which can be caused by volumetric processes in the posterior cranial fossa, damage to the brain stem and cerebellum (including ischemic or toxic) or craniovertebral anomalies [7,8].To clarify the diagnosis according to the indications, laboratory tests were performed (General blood analysis with hemoglobin and erythrocyte levels, glucose level assessment), the study of induced vestibular myogenic potentials, tonal threshold audiometry, caloric test, impedansometry, electrocochleography, posturography or stabilometry, ultrasound duplex scanning of brachiocephalic arteries, magnetic resonance (MRI) or x-ray computed tomography of the brain.The diagnosis was established on the basis of the analysis of complaints, anamnesis of the disease, the results of clinical, laboratory and instrumental examination. The most common and accepted diagnostic criteria in the literature were used. In particular, the diagnosis of PPDB was established on the basis of the characteristic clinical picture, as well as the detection of typical positional nystagmus in positional tests [8].
3. Results and Discussion
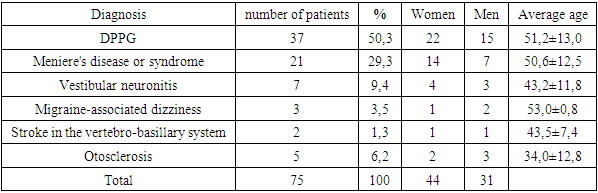
- The clinical diagnoses established in 75 patients analyzed by us, who turned to an outpatient appointment with a neurologist complaining of dizziness, are presented in the table 1.
|
4. Conclusions
- Our study showed that the most common causes of systemic dizziness are diseases of the peripheral vestibular apparatus. In contrast, Central vestibular disorders are relatively rare. The optimal algorithm for clinical examination of patients with vertigo, which allows to identify the most common causes of dizziness and suspect life-threatening Central vestibular disorders, should include, in addition to the standard study of neurological status, the Dix—Hallpike positional test, head shaking test, halmagi test and approximate evaluation of hearing. The use of these methods of clinical examination in ambulatory patients with complaints of dizziness allows without additional instrumental research to diagnose most causes of dizziness and differentiate damage to the Central and peripheral parts of the vestibular analyzer.