Daminov Feruz Asatullaevich
Samarkand State Medical University, Samarkand, Uzbekistan
Correspondence to: Daminov Feruz Asatullaevich, Samarkand State Medical University, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Introduction. The growth of the population of elderly and old people leads to an increase in the need for medical and social assistance. This means that, ceteris paribus, the need for financial resources for the country's health care associated with the treatment of older people will increase significantly. According to statistics, most people die not from old age, but from diseases. Therefore, issues of prevention and treatment of diseases, including burns, which are one of the most common among the elderly and senile, are of great relevance. Purpose of the study: To study the characteristics of disorders of the cardiovascular system in elderly and senile people, depending on the severity of burn shock. Materials and research methods. To achieve the goals and objectives of the study, data on a total of 522 burn victims were used. 2 groups were formed. They were comparable in terms of deep burn area, age and gender. The first group included 217 patients who were treated in the burn department of the Samarkand branch of the RSCEM from 1999 to 2010. Conclusions. Based on this, low and normal CVP values with a fall in blood pressure and severe ECG disturbances testified more to the weakness of cardiac activity than to insufficient infusion-transfusion therapy, and the administration of a large amount of fluid against this background led to decompensation of cardiac activity, which was expressed in overload of the pulmonary circulation, increased CVP.
Keywords:
Burn disease, Senile age, Complications, Course features
Cite this paper: Daminov Feruz Asatullaevich, Characteristics of Disorders of the Cardiovascular System in Elderly and Old Age Persons Depending on the Severity of Burn Shock, American Journal of Medicine and Medical Sciences, Vol. 13 No. 8, 2023, pp. 1102-1106. doi: 10.5923/j.ajmms.20231308.15.
1. Introduction
The growth of the population of elderly and old people leads to an increase in the need for medical and social assistance. This means that, ceteris paribus, the need for financial resources for the country's health care associated with the treatment of older people will increase significantly [2,6]. According to statistics, most people die not from old age, but from diseases. Therefore, issues of prevention and treatment of diseases, including burns, which are one of the most common among the elderly and senile, are of great relevance [1,8,10]. It should be noted that recently there has been a trend towards an increase in the number of victims of thermal injury among the elderly and old people. According to various authors, from 13.3 to 32.7% of patients with burn disease are elderly and senile people [4,6,7,12]. trauma after 60 years is often characterized by a severe course, various complications and adverse outcomes increase. There are also features in the pathogenesis of burn disease in the elderly [5,8,9]. Burn disease has a complex multicomponent pathogenesis, the individual links of which become predominant in different time periods after receiving a burn - hypovolemia and circulatory disorders, especially microcirculation, on the first day after receiving a burn, pronounced intoxication in the first 1-2 weeks, infection in the following weeks [3,10,11].
2. Purpose of the Study
To study the characteristics of disorders of the cardiovascular system in elderly and senile people, depending on the severity of burn shock.
3. Materials and Research Methods
To achieve the goals and objectives of the study, data on a total of 522 burn victims were used. 2 groups were formed. They were comparable in terms of deep burn area, age and gender. The first group included 217 patients who were treated in the burn department of the Samarkand branch of the RSCEM from 1999 to 2010. An in-depth study was conducted in 206 people, the data on which revealed the immediate objectives of the study. The second (control) group included 305 victims with burns treated in the interregional burn center of Samarkand in 1985-1998.
4. Research Results
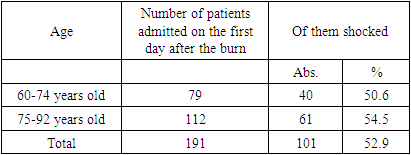
The problem of studying the course of burn shock in elderly and senile patients is one of the most difficult in combustiology.Out of 217 patients treated with burns in the SF RRCEMMP, signs of shock were detected in 101 (52.9%) elderly patients admitted on the first day after injury (191). There were 40 men (39.6%), women - 61 (60.4%). The frequency of burn shock depending on the age of the patients is shown in Table 1.Table 1. The frequency of burn shock depending on the age of the victims
 |
| |
|
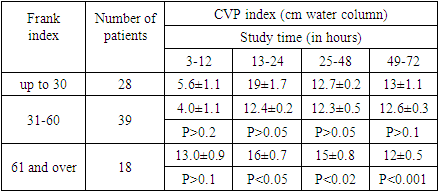
As can be seen from the data in the table, among the elderly who were admitted with burns on the first day after the burn, from 50,6 to 54,5%, depending on age, the state of burn shock was diagnosed.Burn shock is a symptom complex, which is based on extensive thermal damage to the skin and deep tissues, leading to severe hemodynamic disorders with a predominant violation of microcirculation and metabolic processes in the body of the burned person. The leading factors in the development of shock are area and to characterize disorders of the cardiovascular system in elderly and senile people, depending on the severity of burn shock, we studied a number of indicators reflecting the state of the heart and blood vessels (electrocardiography, Echo-ECG, central venous pressure, blood flow velocity, pulse, arterial pressure).During the period of shock, the parameters of pulse, blood pressure (BP) were studied in 101 victims, who were divided into three groups according to the severity of the burn injury.In the first group (30 patients) with the mildest burns (IF up to 30), it did not cause significant hemodynamic disturbances and in 29 people it was well compensated by the circulatory system. At the same time, a moderate heart rate (HR) was observed in 18 (60%) patients, a slight increase in systolic and diastolic blood pressure was observed only in 2 (6.6%) patients.On the second day, both systolic and diastolic blood pressure were within normal limits.In the second group of 44 patients with burns with IF from 31 to 60 on the first day after the burn, a more pronounced decrease in systolic pressure was noted, which in 31 of 44 victims was 25-30% below the age norm and averaged 100 ± 8.8 mmHg. (P<0.01). The value of diastolic pressure at the same time decreased only by 6-8% of the age norm, remaining at the level of 75±3.5 mm Hg.On the second day, systolic blood pressure averaged 120 ± 10.5 mm Hg, and diastolic - 75.5 ± 7.6 mm Hg, while pulse pressure decreased to 45 ± 5 mm Hg.On the third day after the injury in the study group of patients, the systolic pressure increased slightly, on average, to 125.5±7.0 mm Hg, and the diastolic pressure remained practically unchanged and equaled 78.5±6.0 mm Hg. Pulse pressure was 50.0±3.5 mm Hg. In 8 patients of this group, systolic pressure at admission reached 160±10.5 mm Hg, and diastolic 95±4.0 mm Hg. However, the history of hypertension in these patients (according to the anamnesis, their blood pressure ranged from 180/110 to 200/115 mm Hg) gives grounds to conclude that the burn injury in them also led to a decrease in blood pressure.In the third group of 27 patients with IF 61 or more, blood pressure indicators were reduced even more - by 40-45% of the age norm.So, on the first and subsequent days, systolic blood pressure, despite antishock therapy, decreased to 100±7.5 mm Hg, and diastolic blood pressure to 55,5±3,5 mm Hg. (P<0.01), while the pulse pressure was at the level of 45,5±3,0 mm Hg.Significant hypotension persisted on the third day, when systolic pressure decreased to 95±5.5 mm Hg, and diastolic pressure to 60±3.0 mm Hg. The most decrease in blood pressure was observed in 6 victims of this group with extensive deep burns, who died by the end of the first day.Their systolic blood pressure averaged 75,5±5.0 mm Hg, and their diastolic blood pressure was 45,5±2.0 mm Hg. Only in 5 patients from the examined group, systolic blood pressure remained at the level of 120±10 mm Hg. Prior to the burn injury, these patients were treated for coronary artery disease and hypertension, while their blood pressure was kept within 180/100 mm Hg.As can be seen from the study data, a decrease in blood pressure was observed in the group of elderly and senile patients already with mild burn shock (IF up to 30), it decreased even more in patients with severe and extremely severe burn shock. It should be noted that if in the first and second groups of patients hypotension was of a transient nature, then in the group of patients with severe burn shock, blood pressure indicators remained significantly reduced even by the end of the third - the beginning of the fourth day.The relative stability of diastolic pressure in patients on the first day after injury, especially in the group of patients with milder burns, may be associated with a decrease in vascular elasticity due to the atherosclerotic process in this group of patients.An equally important indicator reflecting the state of the cardiovascular system and hemodynamics is the central venous pressure (CVP). The normal figures of which range from 6-12 cm of water. Art. Without CVP measurement, it is impossible to adequately correct the development of a latent or overt shock state. Central venous pressure during the period of burn shock was studied in 85 victims aged 60 years and older. For the purpose of comparative analysis of the effect of burn injury severity on this indicator, patients were divided into the same groups according to the Frank index as in the study of blood pressure indicators.The first group included 28 patients with burns with a Frank index of up to 30, the second group included 31 to 60 burns, and the third group consisted of 18 patients with a Frank index of 61 or more.In the first group of patients, when they were admitted to the hospital, the CVP averaged 5,6±1.1 cm of water. Art., rising by the end of the day to 19 ± 1,7 cm of water. Art. Only in two victims, the CVP remained within the normal range. On the following day, in all patients, the indicators of central venous pressure remained elevated, averaging 12,7±0.2 cm of water. Art., and in one patient the increase reached 12,1 cm of water. Art. By the end of the third day, there was a decrease in CVP to 13±1.1 cm of water. Art., however, in two victims with signs of cardiovascular insufficiency (acrocyanosis, shortness of breath, tachycardia), its indicators remained at the level of 11,8 cm of water.In the group of victims with the Frank index from 31 to 60, the CVP in the first hours after the injury was 4±1.1 cm of water. Art. Only in two patients, CVP indicators were increased to 11.3 cm of water. Art. These patients had severe concomitant diseases of the heart and lungs (coronary cardiosclerosis, pneumosclerosis). By the end of the first day, the value of CVP increased sharply, averaging 12,4±0.2 cm of water. Art. On the second day, the CVP remained elevated to 12,3±0.5 cm of water. Art. In two patients, its value reached 19 cm of water. Art. During the third day, CVP continued to be elevated in comparison with the age norm, amounting to 16±1.3 cm of water. Art. One victim from this group died with symptoms of acute heart failure.Measurement of CVP in patients who had the most extensive and deep burns with a Frank index of 61 or more showed that in the first hours after the burn, its value was the most reduced and averaged 3 ± 0.9 cm of water. Art. In three patients, CVP indices were within 6-7 cm of water. Art., while in one patient it was observed to fall to 13 cm of water. Art. By the end of the day, all victims showed an increase in CVP to 16±0.7 cm of water. On the second day, CVP indicators remained elevated, reaching 19 cm of water in three patients. Art., two of which died without leaving the state of shock. During the third day, the CVP remained at the level of 12±0.5 cm of water. Art., only in two patients its indicators ranged from 15 to 16 cm of water. Art. The nature of CVP changes depending on the severity of the burn shock and the time elapsed since the injury is shown in table 2.Table 2. Change in CVP indicators during the period of burn shock (M ± m)
 |
| |
|
Analyzing the parameters of CVP during the period of shock, it should be noted that the more severe the burn injury, the more pronounced the changes in CVP, while its more significant increase was observed on the second and third days in the group of patients with a Frank index of 61 or more. A decrease in CVP in the first hours after injury is explained by a decrease in the tone of venous vessels, as well as microcirculation and hemodynamic disorders. Subsequently, CVP indicators increased sharply, which was due to a weakening of cardiac activity, as well as overload of the vascular bed with the introduction of infusion-transfusion media, which quickly sets in due to the low compensatory capabilities of the cardiovascular system in this group of patients.Therefore, at low blood pressure, an increase in CVP has always been a poor prognostic sign, indicating the possibility of pulmonary edema.During the period of burn shock, the linear velocity of blood flow changed significantly, the parameters of which depend mainly on myocardial contractility, vascular tone, circulating blood volume and its rheological properties.A study of blood flow velocity in 30 patients over 60 years of age with varying severity of burn shock showed that even in the group of patients with a Frank index of up to 30, it slowed down (table 3).Table 3. Changes in blood flow velocity indicators during the period of burn shock
 |
| |
|
As can be seen from Table 3, the greatest deceleration of the blood flow velocity is noted on the first day, subsequently it was less pronounced, however, in patients with severe burn shock, the blood flow velocity remained slow even by the end of the third day. Apparently, the antishock therapy, in particular, an increase in the volume of circulating blood due to the introduction of fluids, has the greatest effect on the normalization of blood flow velocity.The rate of blood flow also depends on the severity of hemoconcentration, which was studied during this period of burn disease in 60 patients.An increase in hematocrit was detected in 56 out of 60 examined patients, however, we did not observe high hematocrit values even in victims with extensive burns (Frank index 61 or more). Yes, at 21 in a patient with a Frank index of up to 30, the hematocrit indicators increased slightly, amounting to 52±0.04% on the first day and decreased to 43±0.03% by the end of the third day.In the second group of 15 victims with the Frank index from 31 to 60, the hematocrit level reached 57±0.05% on the first day, decreasing to 45±0.04% by the end of the third day.The greatest increase in hematocrit was observed in the last group of 24 patients with a Frank index of 61 or more, where it reached 59 ± 0.05%; as antishock therapy was carried out, the hematocrit value approached the upper limit of normal. Elevated hematocrit numbers, along with other indicators, indicated the severity of the burn injury and served as a rationale for infusion-transfusion therapy for the purpose of hemodilution.Along with the study of blood pressure, CVP, blood flow velocity, hematocrit, which make it possible to judge the state of hemodynamics and the cardiovascular system, in 72 victims during the period of shock, the electrical activity of the heart was studied, which makes it possible to evaluate the following myocardial functions: automatism , excitation and conduction, on the basis of changes in these functions, according to ECG data, one can also judge about organic disorders that underlie functional shifts.Studies have shown that in 7 out of 25 patients with a Frank index up to 30, there was a deviation of the heart axis to the left, in the group of patients with a Frank index from 31 to 60, a levogram was detected in 16 out of 32 victims and in the third group with a Frank index of 61 or more, a deviation of the heart axis to the left observed in 11 of 15 patients.Low voltage of ECG waves in the first group of victims was noted in 12 cases, high P wave in 9 patients, depression of the S - T interval was in 15, an increase in the systolic index in 21, a decrease in the T wave was detected in all victims, including five patients. was negative.In the group of patients with a Frank index from 31 to 60, low voltage of ECG teeth was in 19 burnt patients, a high or jagged P wave was noted in 12 victims, a decrease in the S - T interval was in 16, an increase in the systolic index in 18, a change in the T wave in In 17 patients and in 4 patients, the T wave was negative. 8 patients had atrial fibrillation.All patients with the most severe burns (Frank index 61 or more) had sinus tachycardia, a decrease in the voltage of the teeth, and a deviation of the heart axis to the left. A high P wave or its widening was noted in 10 patients, depression of the interval S -T - in 14 patients, an increase in the systolic index in 7 patients. The T wave was negative in three patients and its decrease was observed in 12 victims. Two victims had atrial fibrillation (table 4).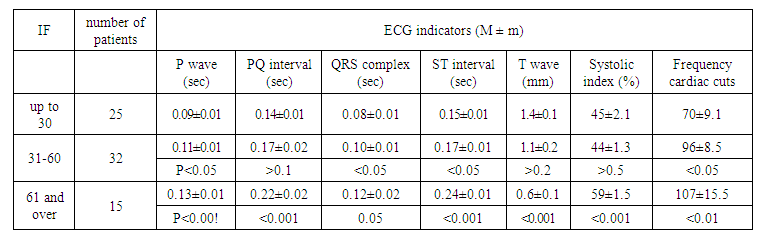 | Table 4. Changes in ECG parameters during the period of burn shock |
Thus, in 56 out of 72 patients during the period of shock, there was a decrease in the voltage of the ECG waves, which indicated the presence of hypoxia, a violation of repolarization and depolarization processes. This was confirmed by depression of the S - T interval, which was found in most patients. It is known that depression of the S - T interval and a decrease in the T wave indicate diffuse myocardial disorders, while at the same time, a change in the T wave can also be associated with local myocardial damage. In these cases, the picture of diffuse disorders is replaced by signs of ischemia and vice versa. An example of this in our studies was the ECG indicators obtained from 9 victims, where there was a depression of the S - T interval and a decrease in the T wave down to a negative one. Three of them had a myocardial infarction, which was the cause of their death, which was confirmed at autopsy. In 6 patients, signs of ischemia were the result of diffuse changes in the myocardium, however, the term "diffuse changes in the myocardium" always indicates pathological changes in the myocardium, expressed to one degree or another.The increase in the P wave or its widening in 31 patients almost always indicated an overload of the right heart and congestion in the pulmonary circulation, caused not only by the impact of a burn injury, but also by concomitant diseases of the heart and lungs. At the same time, there was a danger of developing pulmonary edema, which required a particularly careful approach when conducting fluid therapy in this group of patients.
5. Conclusions
For the most complete assessment of the state of the cardiovascular system, we compared the data on blood pressure, CVP, blood flow velocity and ECG. It was noted that at low blood pressure and pronounced ECG changes, indicating myocardial hypoxia and impaired repolarization processes, intensive transfusion therapy caused the most dramatic increase in CVP, which was clinically accompanied by the appearance of moist rales in the lungs, shortness of breath, and acrocyanosis. Based on this, low and normal CVP values with a fall in blood pressure and severe ECG disturbances testified more to the weakness of cardiac activity than to insufficient infusion-transfusion therapy, and the administration of a large amount of fluid against this background led to decompensation of cardiac activity, which was expressed in overload of the pulmonary circulation, increased CVP.
References
| [1] | Abdurakhmanovich A. A. et al. Pathogenesis, Clinic and Principles of Treatment of Burn Shock // Eurasian Research Bulletin. – 2022. – Т. 9. – С. 20-25. |
| [2] | Arlati S. et al. Decreased fluid volume to reduce organ damage: a new approach to burn shock resuscitation? A preliminary study // Resuscitation. – 2007. – Т. 72. – №. 3. – С. 371-378. |
| [3] | Asadullaevich D. F. Some aspects aggressing burn disease in elderly and senile patients // International Journal of Medical Sciences And Clinical Research. – 2023. – Т. 3. – №. 06. – С. 21-29. |
| [4] | Asadullayevich D. F. et al. Optimization of surgical treatment of early deep burn // Research Focus International Scientific Journal. – 2023. – Т. 2. – №. 4. – С. 234-237. |
| [5] | Cartotto R., Burmeister D. M., Kubasiak J. C. Burn shock and resuscitation: review and state of the science // Journal of Burn Care & Research. – 2022. – Т. 43. – №. 3. – С. 567-585. |
| [6] | Daminov F. A., Karabaev K. K., Khursanov Yo. E. Principles of local treatment of burn wars in hard-burned people // Research Focus. – 2022. – Т. 1. – №. 3. – С. 133-142. |
| [7] | Karabaev H. K. et al. Burn injury in elderly and old age persons // Art of Medicine. International Medical Scientific Journal. – 2022. – Т. 2. – №. 1. |
| [8] | Malik A. et al. Hypertension-related knowledge, practice and drug adherence among inpatients of a hospital in Samarkand, Uzbekistan // Nagoya journal of medical science. – 2014. – Т. 76. – №. 3-4. – С. 255. |
| [9] | Neff L. P., Allman J. M., Holmes J. H. The use of therapeutic plasma exchange (TPE) in the setting of refractory burn shock // Burns. – 2010. – Т. 36. – №. 3. – С. 372-378. |
| [10] | Ruziboev S. A., Daminov F. A. Our experience in treatment of stress ultrasound in severe burned // Euro-Asia Conferences. – 2021. – Т. 1. – №. 1. – С. 447-449. |
| [11] | Vaughn L., Beckel N., Walters P. Severe burn injury, burn shock, and smoke inhalation injury in small animals. Part 2: diagnosis, therapy, complications, and prognosis // Journal of Veterinary Emergency and Critical Care. – 2012. – Т. 22. – №. 2. – С. 187-200. |
| [12] | Yunusov O. T., Daminov F. A., Karabaev H. K. Efficiency of Heprocel in Treatment of Patients with Deep Burns // American Journal of Medicine and Medical Sciences. – 2020. – Т. 10. – №. 8. – С. 624-626. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML