-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2023; 13(7): 1026-1029
doi:10.5923/j.ajmms.20231307.38
Received: Jul. 7, 2023; Accepted: Jul. 22, 2023; Published: Jul. 27, 2023

Anti-Adhesive Barriers in Abdominal Surgery: Our Experience in Minimally Invasive Methods
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRuziboyev Sanjar Abdusalomovich1, Mardonov Vohid Narsullayevich2
1Samarkand State Medical University, Samarkand, Uzbekistan.
2Samarkand branch of the Republican Scientific Center for Emergency Medical Care, Samarkand, Uzbekistan
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The studied results of the treatment of patients with spinal disease of abdominal organs, the determined frequency of relapses of spinal intestinal obstruction and the possibility of laparoscopic adgeziolysis in the surgical treatment of acute spinal intestinal obstruction with the use of the anti-spain barrier agent Hemoben. laparotomy adheziolysis - 539, intestinal resection laparotomy with interintestinal anastomosis-246, intestinal resection laparotomy with excretion of intestinal fistula-88, laparoscopy adhesiolysis-114, which was 11.5% (987) operations due to AAIB. The use of laparoscopic adhesiolysis with the use of anti-adhesion barrier agent Gemoben promotes early recovery of intestinal motility, reduces the frequency of recurrence of adhesive pain, and reduces the duration of hospitalization.
Keywords: Adhesive intestinal obstruction, Laparoscopic adhesiolysis
Cite this paper: Ruziboyev Sanjar Abdusalomovich, Mardonov Vohid Narsullayevich, Anti-Adhesive Barriers in Abdominal Surgery: Our Experience in Minimally Invasive Methods, American Journal of Medicine and Medical Sciences, Vol. 13 No. 7, 2023, pp. 1026-1029. doi: 10.5923/j.ajmms.20231307.38.
1. Introduction
- Analysis of the foreign and nationalliterature showed that video laparoscopic surgeryaimed to eliminate the cause of the intestinal contents passage disturbance have significant advantages over the traditional laparotomy intervention with the different approach to the choice of treatment method and correct selection of patients for the operation which ultimately helps to achieve the best quality of their life. Acute adhesive intestinal obstruction (AAIO) remains a difficult problem of emergency abdominal surgery due to difficulties in its diagnosis and treatment, absence of effective methods of prevention, significant percentage of complications, high mortality rate and financial costs [1,2]. Confirming the international status of the problem, the International Adhesions Society (IAS) was formed in Dallas, Texas, USA, in 1996. Surgical interventions for adhesions of abdominal cavity do not exclude the possibility of recurrence, and sometimes are the stimulating factor of adhesion formation [13,18,19,20]. Adhesiolysis during laparotomy is not a guarantee of their absence in the future. According to some data, recurrences occur in up to 50% of cases; repeated surgeries increase the risk of adhesions formation and their complications [3,4,5,7,8]. Currently, there is a tendency of video laparoscopy application in the treatment of adhesive intestinal obstruction. According to the data of domestic and foreign authors, the method reduces the patients' stay in the hospital and decreases the number of complications.According to a number of authors, the proportion of laparoscopic operations varies from 11.4 [6,9,17] to 97.0% [14,15,21]. There are a number of works describing clear advantages of laparoscopic operations for acute intestinal obstruction in comparison with open operations [9,10]. Thus, the number of complications after laparoscopic operations performed is by 25% lower than after open surgeries [11,12,16]. Such difference in the frequency of laparoscopy use can indicate significant differences in the choice of indications for laparoscopic surgery in UCI or insufficiently clear guidelines.Objective. To study the possibilities of laparoscopic adhesiolysis in surgical treatment of acute adhesive intestinal obstruction, decreasing of frequency of recurrences of adhesive intestinal obstruction and also to determine the use of modern barrier means for complex of anti-adhesive measures.
2. Materials and Methods
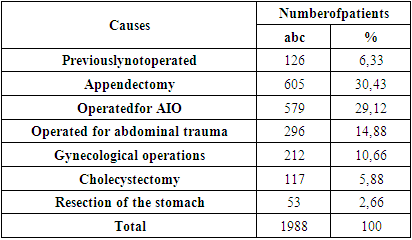
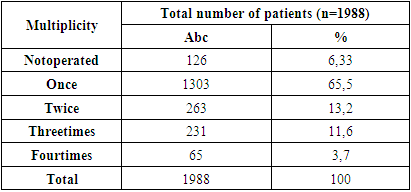
- Nowadays 114 attempts of minimally invasive operations concerning acute adhesive intestinal obstruction were carried out: 89 at the onset of the attack for urgent indications, and 25 - after ileus medicalization in a planned procedure. Complex of conservative measures, conducted parallel with diagnostic manipulations included: nasogastric drainage, infusion therapy, injections of antispasmodics, anticholinesterase agents, setting of hypertonic and purging enemas. For comparison of efficiency of the laparoscopic adhesiolysis we analyzed results of treatment of 1988 patients with acute intestinal obstruction in Samarkand branch of Republican Scientific Center of Emergency Medical Careduring the period from 2010 till 2022. 1286 patients (64,7%) were diagnosed with small intestinal obstruction from the total number of patients, 702 (35,3%) patients had colonic obstruction. Operative treatment was used in 987 patients (49,6%), from them 706 (71,5%) patients had small-intestinal and 281 patients had colonic obstruction. The most frequent causes of adhesive intestinal obstruction are given in Table 1.
|
|
3. Results and Discussion
- At admission all patients underwent clinical and biochemical blood tests, X-ray examination, ECG, ultrasound of the abdominal cavity organs and diagnostic laparoscopy, and multispiral computer tomography if necessary. Type of operative interventions: laparotomy-adhesiolisis-539, laparotomy-intestinal resection with interintestinal anastomosis- 246, laparotomy-intestinal resection with fistula withdrawal-88, laparoscopy-adhesiolisis-114, which was 11.5% (987) of operations for acute adhesive intestinal obstruction in 2010-2022. During the operation we are faced with various optionsof adhesions and divided into the following groups: single coarse cord-like adhesions were detected in 57 patients (after laparoscopic operations), multiple flat visceral-parietal in 39 patients, mixed armored abdomen in 18 patients. The conversion rate is 18%. The main reasons of conversion were technical difficulties at separation of adhesions and conglomerates of the adherent small intestine loops, intestinal necrosis or traumatic damage of the intestinal wall. If necessary, patients underwent peridural block, which allowed to restore motility of the intestinal tract within the next 2 days.
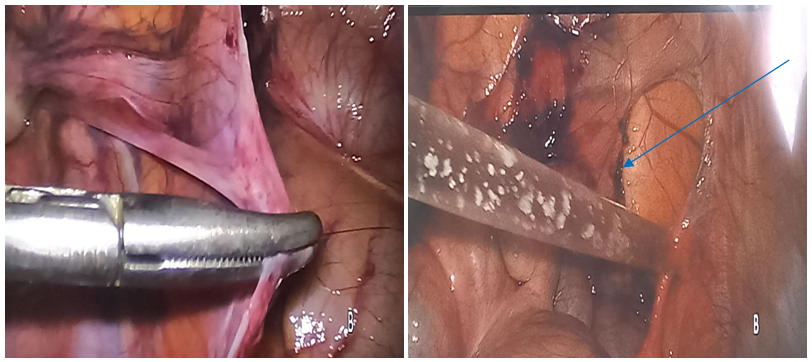 | Picture 1. Dissection of adhesions and the use of PSB "Hemoben" аnd methylene blue |
4. Conclusions
- 1. Laparoscopic adhesiolysis with the application of antispastic barrier agents is advisable to be performed in patients with I-II degree adhesions in whom AAIO was stopped by conservative measures.2. Mini laparotomy is pathogenetically reasonable in case of technical difficulties during laparoscopic adhesiolysis; laparotomy is recommended in degree IV adhesions. 3. After adhesiolysis a complex of anti - adhesivemeasures with the use of systemic enzymotherapy preparations is indicated. 4. Modern anti - adhesivebarriers are the key to successful surgical treatment of abdominal adhesions irrespective of the method of operation as they are pathogenetically grounded approach to the prevention of disease recurrence.