-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2023; 13(7): 955-957
doi:10.5923/j.ajmms.20231307.24
Received: Jul. 10, 2023; Accepted: Jul. 21, 2023; Published: Jul. 24, 2023

Clinical and Diagnostic Criteria of Myocarditis Associated with COVID-19 in Pregnant Women
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLD. D. Eshonkhodjaeva1, N. A. Urinbaeva2
1Tashkent State Dental Institute, Tashkent, Uzbekistan
2Republican Perinatal Center, Tashkent, Uzbekistan
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of the research was to study the role of COVID-19 viral infection during pregnancy on the development of myocarditis in pregnant women and on the course of pregnancy and childbirth. Background. COVID-19 is mainly a respiratory infection, however, in some cases, it can lead to cardiac complications in pregnant women - the development of myocarditis. Material and methods. A total of 147 pregnant women with myocarditis were examined: 95 women who underwent COVID-19 and 52 pregnant women with chronic focal myocarditis. The following instrumental investigations were carried out: echocardiogram, ultrasound with Doppler uteroplacental-fetal blood flow. Mean age of the examined patients was 28.7±5.2 years. Results. Echocardiography in group 1 pregnant women revealed mitral or tricuspid regurgitation (68%), mitral or tricuspid insufficiency (61%) significantly more often (P<0.05). In patients of group 2 on ECHOCG diastolic dysfunction of the left ventricle was determined almost 2 times more often (p<0.01) compared with pregnant women of group 1. Conclusion. COVID-19 associated myocarditis in pregnant women develops mainly 3-4 weeks after COVID-19. Timely diagnosis of myocarditis associated with COVID-19 in pregnant women allows for treatment and reduces the frequency of complications and operative delivery.
Keywords: COVID-19, Pregnancy, Myocarditis, Treatment
Cite this paper: D. D. Eshonkhodjaeva, N. A. Urinbaeva, Clinical and Diagnostic Criteria of Myocarditis Associated with COVID-19 in Pregnant Women, American Journal of Medicine and Medical Sciences, Vol. 13 No. 7, 2023, pp. 955-957. doi: 10.5923/j.ajmms.20231307.24.
1. Introduction
- Reducing maternal mortality is a global goal of the World Health Organization (WHO). Although maternal mortality due to bleeding and infection is decreasing, cardiovascular-related lethality is increasing and is currently the most important cause in many countries of the world.The COVID-19 coronavirus pandemic has made its own adjustments to the nature of the pregnancy course. The first publications on the course of pregnancy in women who underwent COVID-19 during gestation showed that pregnant women carried it more often in a mild form. Pregnancy is a partially immunodeficient condition and therefore pregnant women are more susceptible to the development of viral diseases. The Guidelines, published by the Society of Cardiologists of Great Britain, provide data on cardiovascular diseases congenital or acquired during pregnancy [1]. At the same time, pregnant women have complaints of dyspnea and lack of air, which may mean that there is a risk of cardiac decompensation and can lead to life-threatening consequences for the mother and the unborn child. The most common cause of a deterioration in the condition of a pregnant woman after a cold is hypertensive disorders, preeclampsia, against which there are signs of a violation of the cardiovascular system [2-4]. At the same time, the clinic of myocarditis after COVID-19 is not typical and is often considered a complication of preeclampsia. Viral infections in pregnant women can lead to the development of myocarditis within a few days or up to 3 months after an infectious and inflammatory disease. Clinical studies have established that cardiotropic virus, being an etiological factor, induces activation of cellular and humoral immunity and inflammatory injury to myocardial tissue mediated by immune reactions in the form of delayed hypersensitivity reactions. Most viruses are phagocytized and excreted from the body within 10-14 days. At the same time, nucleic metabolism disorders persist in injured myocardial cells, which leads to the development of IgG class antibodies that react with intact cardiomyocytes, triggering autoimmune processes. Myocarditis is developed a few weeks after the initial infection and the injury to the myocardium is infectious and allergic in nature [5].The last year and a half are characterized by an increase in the incidence of myocarditis in pregnant women after COVID-19 during gestation, which can lead to complications of pregnancy course [6]. Data on the impact of COVID-19 on the course of pregnancy and the development of complications are currently being studied and summarized.The aim of the research was to study the role of COVID-19 viral infection during pregnancy on the development of myocarditis in pregnant women and on the course of pregnancy and childbirth.
2. Material and Methods
- The studies were carried out at the Republican Perinatal Center in the period from 2.10.2021. to 31.09.2022. We examined 150 pregnant women with myocarditis observed during pregnancy and admitted for childbirth. The age of the examined ranged from 20 to 39 years. Mean age of the examined patients was 28.7±5.2 years. All the examined patients were divided into 2 groups: Group I – 95 pregnant women who had COVID-19 during pregnancy and Group II – 52 pregnant women with myocarditis who did not have COVID-19. The anamnesis, data on the undergone COVID-19 infection, the severity of the disease were studied. The following instrumental investigations were carried out: echocardiogram, ultrasound with Doppler uteroplacental-fetal blood flow. There were no vaccinated patients during pregnancy from COVID-19 among the examined pregnant women. Statistical studies were carried out according to the standard methodology. Differences in the results were considered reliable at p<0.05.
3. Results
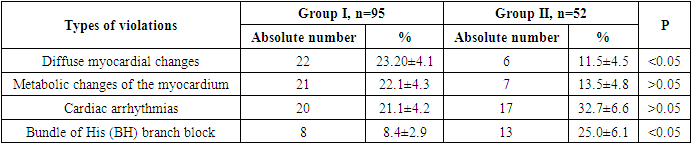
- 65% of pregnant women in Group I had COVID-19 in the I-trimester, in the II-trimester - 35%. In Group I the course of COVID-19 was mild in 71 pregnant women, moderate-severe - in 29 cases. Almost all pregnant women were performed a PCR-test for COVID-19, but it was positive only in half of the examined patients. The rest were diagnosed on the basis of a characteristic pattern – colds, loss of sense of smell, detection of IgM and IgG antibodies to the COVID-19 virus in the blood. Myocarditis was first detected in pregnant women of Group I in the first trimester at 8-12 weeks, and in the second trimester - at 16-26 weeks. A thorough anamnesis revealed that the appearance of signs of myocarditis – dyspnea, pain in the heart area, palpitations, weakness, dizziness - were noted on average 3-4 weeks after the manifestations of COVID-19 [2,6]. In Group II of pregnant women, myocarditis was detected before pregnancy. In the anamnesis, these women had colds, childhood infections in the adult period and rheumatic diseases. All these patients were registered by a cardiologist for chronic sluggish focal myocarditis.The conducted functional studies revealed some differences in the indicators of Groups I and II. Thus, for patients of Group I with newly diagnosed myocarditis associated with COVID-19, diffuse changes were detected on the ECG 2 times more often and metabolic changes of the myocardium - 1.6 times more often than in Group II.On an echocardiogram (EchoCG) in pregnant women of Group I who underwent COVID-19, mitral or tricuspid regurgitation (68%), mitral or tricuspid insufficiency (61%) were significantly more often (p<0.05) detected. At the same time, left ventricle diastolic dysfunction (LVD) on EchoCG in pregnant women of Group I was detected almost 2 times less often (p<0.05) in compare with pregnant women of Group II (Tab.1).
|
4. Discussion
- The course of myocarditis that developed in pregnant women who had COVID-19 in the I-trimester or in the II-trimester is characterized by certain clinical symptoms - weakness, shortness of breath, dizziness, palpitations, characteristic of myocarditis which was developed after influenza, viral and colds after an average of 1.5 - 3 - 4 weeks after illness [2-4]. At the same time, such signs as mitral or tricuspid regurgitation were detected in pregnant women of Group II with chronic focal myocarditis less frequently than in the data of patients of the Group I, which indicates the development of compensatory changes in their body associated with the duration of the disease. The presence of chronic cardiac pathology in pregnant women can lead to an increase in vasoconstriction, an increase in blood pressure, hemostasis system disorders and the development of hypertensive conditions more often than in group 1 pregnant women with COVID-associated myocarditis, which is confirmed by literature data [5,7-8]. Identified blood flow disorders in the fetoplacental complex were also noted more often in pregnant women of Group I, which we associate with hypercoagulability. Timely treatment helped to improve cardiac performance, reduce the incidence of severe preeclampsia, which allowed to reduce the frequency of operative labor and to carry out childbirth through the natural birth canal.
5. Conclusions
- The development and first manifestations of COVID-19-associated myocarditis are detected 3-4 weeks after COVID-19, characterized by signs of circulatory disorders that require consultation of a cardiologist. In pregnant women of Group I, signs of myocarditis on echocardiography had vivid manifestations with a short duration of the disease compared to pregnant women with sluggish focal myocarditis, which was associated with an insufficient degree of compensatory mechanisms development. Timely diagnosis of myocarditis associated with COVID-19 in pregnant women allows to carry out treatment and reduce the frequency of complications and operative delivery.The authors declare no conflict of interest. This study does not include the involvement of any budgetary, grant or other funds. The article is published for the first time and is part of a scientific work.