-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2023; 13(6): 772-774
doi:10.5923/j.ajmms.20231306.02
Received: Apr. 5, 2023; Accepted: May 8, 2023; Published: Jun. 10, 2023

Direct Results of Combined Gastrectomy with Distal Hemipancreatectomy and Splenectomy for Locally Advanced Gastric Cancer
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLA. Kh. Melikulov1, M. D. Dzhuraev2
1Abdominal Onco-Surgeon of the Samarkand Branch of the Republican Specialized Oncology and Radiology Scientific and Practical Medical Center
2Director of the Tashkent City Branch of the Republican Scientific and Practical Medical Center of Specialized Oncology and Radiology
Correspondence to: A. Kh. Melikulov, Abdominal Onco-Surgeon of the Samarkand Branch of the Republican Specialized Oncology and Radiology Scientific and Practical Medical Center.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The direct results of surgical treatment of locally advanced gastric cancer in 47 patients were studied in the article. All of the patients who were operated on were in the T4bN0-2M0 stage. The number of postoperative complications after combined gastrectomy with distal hemipancreatectomy and splenectomy was observed in 8 patients (14.9%). Postoperative mortality was 1 (2.1%).
Keywords: Locally advanced gastric cancer, Combined gastrectomy, Distal hemipancreatectomy
Cite this paper: A. Kh. Melikulov, M. D. Dzhuraev, Direct Results of Combined Gastrectomy with Distal Hemipancreatectomy and Splenectomy for Locally Advanced Gastric Cancer, American Journal of Medicine and Medical Sciences, Vol. 13 No. 6, 2023, pp. 772-774. doi: 10.5923/j.ajmms.20231306.02.
Article Outline
1. Relevance
- Patients with stage I-II gastric cancer account for 10.1%, patients with stage III 61.1%, and patients with stage IV 28.8% [6]. Men with gastric cancer occupy the first place in oncological diseases in Uzbekistan, at 12.3 percent [4]. Despite a steady trend of morbidity decrease over the last decades, gastric cancer remains one of the most common malignant tumors [2,12]. Combined surgeries in the treatment of gastric cancer are currently widespread. So, in the 1990s of the twentieth century, Japan performed 40% of all surgical interventions, while Europe and the United States performed 20% [14,15]. One of the major issues with stomach cancer is that the majority of patients are admitted to specialized medical treatment facilities with locally advanced processes when the tumor grows into the adjacent organs and tissues, and with this in mind, the surgery has a conventional radical character, which can have no positive effect on the distant survival rate [1,7]. At present, it is considered that the results of gastric cancer treatment can be improved by more aggressive combined operations, the main indication for which is a detectable visual protrusion of the gastric tumor into the adjacent organs in the absence of distant metastases and tumor dissemination through the abdominal cavity [1,8]. Gastrectomy with splenectomy and gastrectomy with distal hemipancreatectomy with splenectomy are the most frequent combined operations in gastric cancer with pancreatic tail [5]. A comparison of immediate and long-term results of combined surgeries is incorrect, because the treatment results are significantly affected by which organ is removed together with the stomach. Most often, the spleen, the tail of the pancreas, the left lobe of the liver, and the head of the pancreas are removed together with the stomach; less often, the diaphragm and the adrenal gland are resected. One organ is resected with the stomach more frequently (71%); two organs are resected less frequently (22%); three or more organs are resected in 7% [9,11]. When studying the literature all over the world on operations of extended combined gastrectomy, the survival rates of patients were as follows: 1-year survival reached 82.5%, 3-year survival reached 44.7%, and 5-year survival reached 19.5%. [3,8,10,13,16].
2. Objective
- To evaluate the immediate results of combined gastrectomies with distal hemipancreatectomy with splenectomy for locally advanced gastric cancer.
3. Material and Methods
- We studied the immediate results of surgical treatment of locally advanced gastric cancer in 17 patients who underwent combined gastrectomy with distal hemipancreatectomy with splenectomy from September 2017 to July 2022 in the department of Thoracoabdominal Surgery of Samarkand branch of RSSPMCOR. The majority of the patients who were operated on were men: 33 (70.2%). According to the age distribution of the patients, the bulk of the patients were 50–70 years old. Adenocarcinomas of various differentiation were found in 38 (80.8%) patients according to the histological structure of the tumor, scarred cancer in 4 (8.5%), and papillary cell cancer in 5 (10.6%) patients. All patients were examined in the preoperative period according to the standard of diagnostics. According to localization of the tumor in the stomach, in 36 (76,6%) patients the primary tumor was localized in the body and proximal part of the stomach with invasion into the caudal part of the pancreas, and in 11 (23,4%) patients there was total involvement of the stomach with partial invasion into the body and caudal part of the pancreas. All of the patients who were operated on were in the T4bN0-2M0 stage. All patients had gastric bleeding of varying intensity, which was an indication for surgical intervention without neoadjuvant chemotherapy.
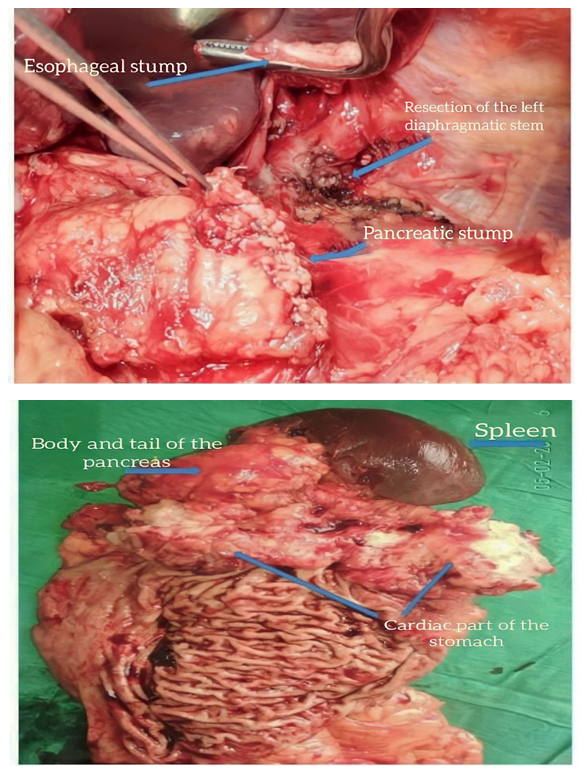 | Figure 1 |
4. Results and Discussions
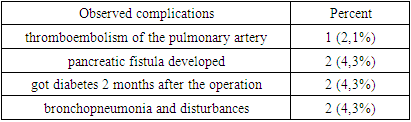
- It is generally recognized that a well-developed technique of surgical intervention for gastric cancer allows for satisfactory immediate results regardless of the volume of the operation performed. In 47 patients, abdominal cavity revision was performed after laparotomy, and dissemination and endramatosis were excluded. The gastroplasty technique remained unchanged. After mobilization of the large curvature of the stomach and determination of the extent of tumor infiltration into the body and tail of the pancreas, the posterior wall of the pancreas was mobilized within the healthy tissue and taken for tourniquet, and the splenic artery and vein were separately ligated along the pancreas. The proximal part of the mobilized pancreas was sutured with UO-60 apparatus, and the pancreatic stump was also treated with continuous atraumatic sutures. Then the distal part of the pancreas and spleen were mobilized, and the tumor was removed in one unit. In the postoperative visit, the main attention was paid to the prescription of antibacterial therapy, the use of enzyme inhibitors, and drugs that reduce pancreatic secretion.The number of postoperative complications after combined gastrectomy with distal hemipancreatectomy with splenectomy was observed in 7 patients (14.9%). Among the surgical complications, 1 (2,1%) patient had a thromboembolism of the pulmonary artery; in 2 (4,3%) cases, a pancreatic fistula developed, which closed automatically within 4 weeks; and in 2 (4,3%) patients, a chronic pancreatitis was diagnosed before the operation, so the patient got diabetes 2 months after the operation. Therapeutic complications were represented in the form of bronchopneumonia and disturbances of cardiac rhythm in 2 patients (4.3%). In both cases, the complications were eliminated by conservative treatment.
|
5. Conclusions
- Thus, it should be emphasized that in the surgical treatment of locoregional gastric cancer, combined gastrectomy with distal hemipancreatectomy and splenectomy does not significantly increase the number of postoperative complications and almost does not differ in the nature of complications from standard gastrectomy. Combined gastrectomy with distal hemipacreatectomy with splenectomy provides radical surgical treatment for locally advanced gastric cancer and, in turn, reduces postoperative recurrence and thereby improves long-term results and the survival rate.