Tukhtaev Firdavs Mukhitdinovich, Mavlyanov Farhod Shavkatovich, Mavlyanov Shavkat Khodzhamkulovich, Tursunov Sanjar Esankulovich
Samarkand State Medical University, Samarkand, Republic of Uzbekistan
Correspondence to: Tukhtaev Firdavs Mukhitdinovich, Samarkand State Medical University, Samarkand, Republic of Uzbekistan.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The number of cases of congenital malformations and diseases of newborns is increasing along with the demographic rise, indicating a problematic situation in modern neonatology and pediatric surgery. In the next decade, the proportion of healthy newborns in the population may decrease to 15-20%. The most common pathology in neonatal surgery is congenital intestinal obstruction, causing a significant number of admissions to surgical hospitals and high mortality rates, but prognostic criteria for the course of the disease and recovery after surgery are not yet well-developed, and there is no consensus on the criteria for starting enteral nutrition. The aim of the study was to analyze the results of complex treatment of 63 newborns with intestinal obstruction, depending on the characteristics of the postoperative period. Materials and Methods. The children were divided into 2 groups. Group 1 included 42 newborns who were postoperatively managed by the traditional method. The second group consisted of 21 children with a feature of postoperative care, which was the use of early enteral nutritional support. The results obtained allow us to state that the use of early enteral nutritional support in the complex of postoperative management of children with congenital intestinal obstruction has a positive effect on the results of surgical intervention. Conclusion. Early enteral nutritional support as part of the postoperative care for children with congenital intestinal obstruction has a positive impact on surgical outcomes, resulting in earlier intestinal peristalsis and reduced occurrence of postoperative complications such as bloating, dysbiosis, and vomiting.
Keywords:
Newborns, Intestinal obstruction, Treatment, Results, Postoperative period
Cite this paper: Tukhtaev Firdavs Mukhitdinovich, Mavlyanov Farhod Shavkatovich, Mavlyanov Shavkat Khodzhamkulovich, Tursunov Sanjar Esankulovich, Analysis of Immediate Results of Surgical Treatment of Children with Congenital Intestinal Obstruction, American Journal of Medicine and Medical Sciences, Vol. 13 No. 5, 2023, pp. 576-580. doi: 10.5923/j.ajmms.20231305.06.
1. Introduction
Together with the demographic rise, an increase in the number of cases of congenital malformations and diseases of newborns is registered, which outline the problematic situation developing in modern neonatology and pediatric surgery. In the next decade, the proportion of healthy newborns in the population may decrease to 15-20%. The most common pathology in neonatal surgery is congenital intestinal obstruction, which is registered with a frequency of 1:2000 newborns. Intestinal obstruction accounts for 1.5-9.4% of all diseases of the abdominal cavity and causes 3-5% of admissions to surgical hospitals. The mortality rate is 3-10%, postoperative in complicated forms reaches 30% and occupies one of the first places among urgent surgical diseases according to this indicator.At the same time, prognostic criteria for the course of intestinal obstruction, leading to the development of local and systemic complications, have not been sufficiently developed to date. In addition, the development of surgery for gastrointestinal malformations in newborns is inevitably accompanied by an increase in the frequency of postoperative complications. There is no single view in the literature on the timing of recovery of passage along the upper gastrointestinal tract in newborns after surgery for intestinal obstruction of obstruction. The data on the criteria for starting enteral nutrition and the possibility of switching to full enteral nutrition are very contradictory.
2. Purpose of the Research
To study the results of surgical treatment in the immediate postoperative period, depending on the features of postoperative management of children with congenital intestinal obstruction.
3. Material and Methods
A prospective study of 63 newborns with intestinal obstruction (OCN) who were examined and treated at the Samarkand Regional Children's Medical Multidisciplinary Center for the period from from January to December 2022 was conducted.According to the classification of Yu.F. Isakov, there were 30 newborns with high intestinal obstruction and 33 with low intestinal obstruction. There were 39 boys and 24 girls. Figure 1.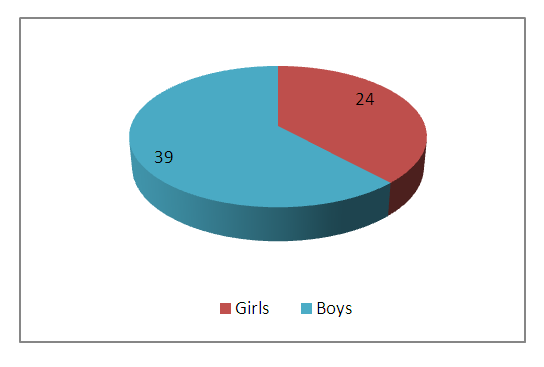 | Figure 1. Gender composition of newborns with intestinal obstruction |
Among the applicants, children of the rural population prevailed, 57 newborns and 6 infants were from the city. Depending on the time of hospitalization, 34 children were under the age of 3 days, from 4 to 10 days there were 24 newborns and from 10 to 20 days – 5 children. Figure 2.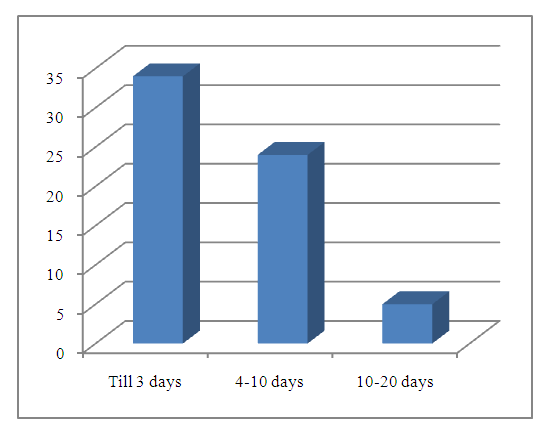 | Figure 2. Age of newborns at the time of hospitalization |
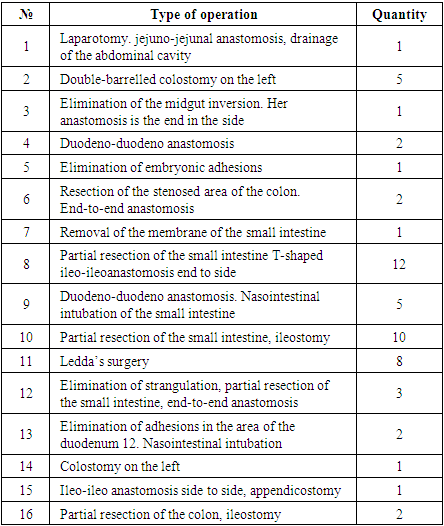
Surgical intervention in 45 newborns with congenital intestinal obstruction (CIO) was performed from the moment of birth to surgery in terms from 1 to 5 days. 2 patients did not undergo surgery due to the parents' refusal of the proposed treatment. The remaining 16 children underwent surgical treatment after 5 days from the moment of birth.From the moment of admission to the hospital before the operation, 54 children with CIO and 7 newborns were operated on within 48 hours at a later date (3 days).61 newborns underwent the following surgical operations. Table 1.Table 1. Types of operations performed by a newborn with congenital intestinal obstruction
 |
| |
|
For the convenience of data interpretation, all children were examined according to a single survey standard. Along with the generally accepted clinical methods, including the analysis of complaints, anamnesis data and objective examination (pulse, respiratory rate, body temperature, urination, etc.), targeted laboratory and instrumental studies were carried out.The next stage of our work was the analysis of the results of complex treatment of newborns with CN, depending on the characteristics of the postoperative period. For this purpose, the children were divided into 2 groups. Group 1 included 42 newborns whose postoperative management was carried out by the traditional method. The second group consisted of 21 children whose special feature of postoperative care was the use of early enteral nutritional support.Complete parenteral nutrition in the postoperative period was carried out in all patients after normalization of homeostasis indicators. In children of group 2, 24 hours after the operation, mixed nutrition (partial enteral + parenteral) was started; the following scheme of enteral nutrition was used: saline solutions were injected through a nasogastric (nasointestinal) probe and, in the presence of evacuation of the full volume, which was noted by the 4th-5th day, non-hydrolyzed mixtures or mother's milk in the starting dose were administered 2 ml/kg, mainly by bolus method.The results of surgical treatment were evaluated according to the following criteria: the timing of the appearance of intestinal peristalsis in the early postoperative period and the presence of postoperative complications such as bloating, vomiting, dysbiosis, peritonitis.
4. Results
The analysis of clinical and diagnostic data allowed to identify complications and concomitant diseases with which newborns with intestinal obstruction were hospitalized before the operation. 39 children without complications were transferred from maternity hospitals, taking into account the rules of transportation of patients with this pathology. 14 patients were hospitalized with severe dehydration, 5 had intraoperative small intestine necrosis. 1 child was admitted with acute respiratory failure on the background of aspiration pneumonia and severe exicosis with toxicosis. 3 children were diagnosed with peritonitis on the background of intestinal obstruction. Figure 3.At admission from concomitant diseases, anemia was most common in 30 children, an open oval window took 2nd place in frequency – 19 newborns, VSD – 1 patient. Intrauterine infection was verified in 6 children with CIO, spontaneous thrombocytopenia was observed in 2 patients. Figure 3.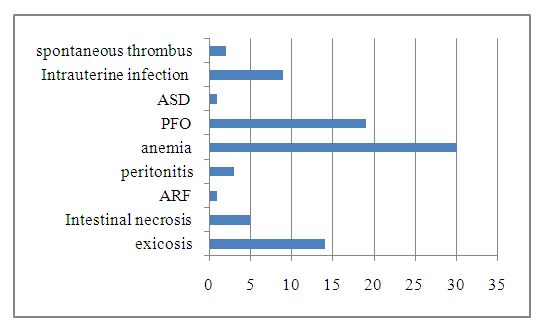 | Figure 3. Types of complications and concomitant diseases in children with CIO before surgery |
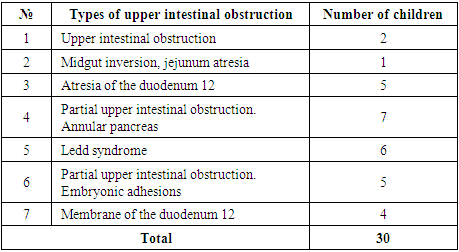
High congenital intestinal obstruction was diagnosed in 30 infants and low in 33 newborns.Boys with upper CIO were 16, girls – 14. Clinical and instrumental diagnostics and intraoperative picture revealed the following types of upper intestinal obstruction in the examined children (Table 2, Figure 4).Table 2. Types of upper intestinal obstruction
 |
| |
|
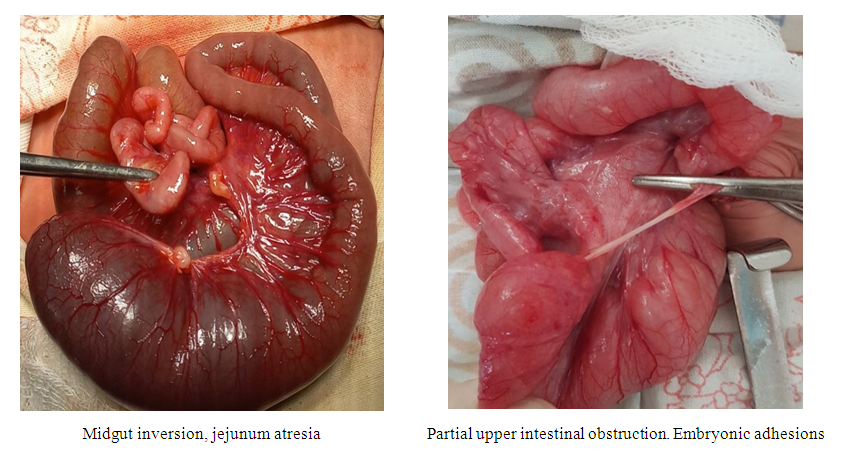 | Figure 4. Types of congenital high intestinal obstruction |
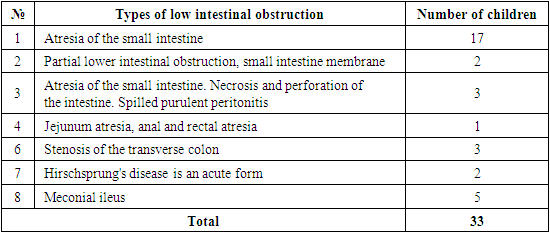
Of 33 newborns with low intestinal obstruction, there were 19 boys and 14 girls. Clinical and instrumental diagnostics and intraoperative picture revealed the following types of lower intestinal obstruction in the examined children (Table 3, Figure 5).Table 3. Types of lower intestinal obstruction
 |
| |
|
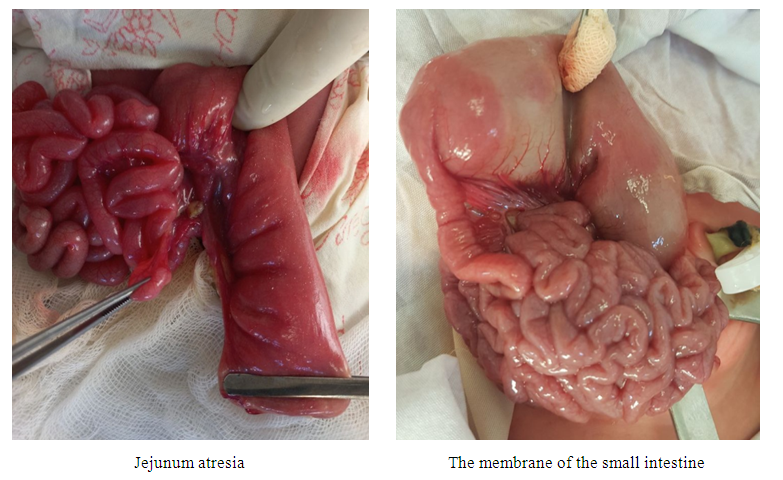 | Figure 5. Types of congenital low intestinal obstruction |
In group 1 patients with traditional postoperative management, intestinal peristalsis was auscultatively listened to 3-4 days after surgery. Of the 42 infants who made up group 1, 80.9% (34 newborns) had intestinal paresis before 6 days in the immediate postoperative period, expressed by bloating, regurgitation, separated through a nasogastric probe of gastrointestinal contents. The discharge of intestinal contents through the ileostomy in this category of patients was noted on 4-5 days after surgery. Fecal masses through a colostomy or during defecation were released on 7-8 days after surgery.In the second group, in which newborns 12-24 hours after surgery, saline solutions were injected through a nasogastric (nasointestinal) probe, and then non-hydrolyzed mixtures or mother's milk, out of 21 infants, in 16 (76.2%), intestinal peristalsis was auscultatively listened to 36-48 hours after surgery. Evacuation of the nutritive agent from the upper gastrointestinal tract to the lower was noted. In all infants included in the second group, the intestinal contents of the small intestine were excreted through the ileostomy on day 2, the contents of the large intestine through the colostomy or in the form of fecal masses during defecation on day 3-4 after surgery. In the immediate postoperative period, intestinal paresis persisted.The study showed that CIO in newborns leads to a lack of microbial diversity. This process predisposes to disruption of the physiological processes of the resident microflora during colonization, the acquisition of antibiotic-resistant strains of microorganisms and the development of inflammatory diseases caused by facultative and transient microflora. In children of group 1, the presence of a prolonged infection of the digestive tract was revealed. Newborns developed dysbiosis, one of the characteristic features of which was colonization of the intestine by pathogenic microorganisms (Figure 6).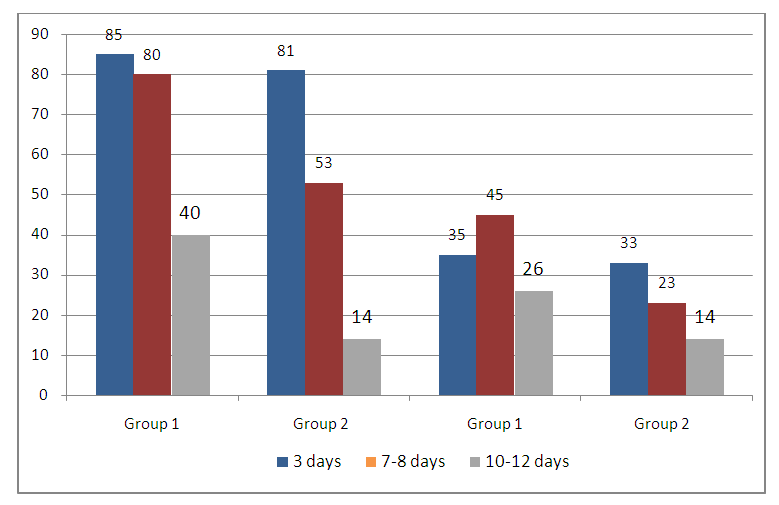 | Figure 6. Frequency of detection of pathogenic intestinal microflora in children with CIO |
As can be seen from Figure 6, on the 7-8 day after surgery, in children of group 2, the use of early nutritional support makes it possible to suppress the growth and development of Staphylococcus spp. and Streptococcus spp.. This is expressed in a significant decrease in the frequency of detection of pathogenic flora in newborns of this group.
5. Conclusions
The results obtained allow us to assert that the use of early enteral nutritional support in the complex of postoperative management of children with CIO positively affects the results of surgical intervention. In children in the early postoperative period, intestinal peristalsis appears much earlier and such postoperative complications as bloating, dysbiosis, vomiting are much less common.
References
| [1] | Власов А. П., Трофимов В. А., Григорьева Т. И. и др. Энтеральный дистресс-синдром в хирургии: понятие, патогенез, диагностика // Хирургия. 2016. No 11. C. 48–53. |
| [2] | Ф. Мавлянов, Ш. Мавлянов, С. Турсунов, У. Баратов Пути улучшения результатов лечения детей с врождённой кишечной непроходимостью // Детская хирургия 2021 Том 25 Номер S1 С.51. |
| [3] | Хирургические болезни детского возраста. Учебник. Под редакцией Ю.Ф. Исакова. Том 1. 2004г. стр. 302. |
| [4] | Bethell G.S. Long A.M. Knight M. Hall N.J. Congenital duodenal obstruction in the UK: a population-based study. Arch Dis Child: Fetal Neonatal editor. 2020; 105: F178-F183. |
| [5] | Peng Y.F. Zheng H.Q. Zhang H. He Q.M. Wang Z. Zhong W. et al. Comparison of outcomes following three surgical techniques for patients with severe Jejunoileal Atresia. Gastroenterol Rep (Oxf). 2019; 7: 444-448. |
| [6] | Laurens D. Eeftinck Schattenkerk, Manouk Backes, Wouter J. de Jonge, Ernest LW. van Heurn, Joep PM. Derikx Treatment of jejunoileal atresia by primary anastomosis or enterostomy: Double the operations, double the risk of complications Jourmal of Pediatric surgery Vol 57, ISSUE 9, P49-54, September 2022. |
| [7] | Kinlin C. Shawyer AC. The surgical management of malrotation: a Canadian association of pediatric surgeons survey. J Pediatr Surg. 2017; 52: 853-858. |
| [8] | Rebecca A. Saberi, Gareth P. Gilna, Blaire V. Slavin, Eduardo A. Perez, Juan E. Sola, Chad M. Thorson Outcomes for Ladd's procedure: Does approach matter? Jourmal of Pediatric surgery Vol 57, ISSUE 1, P141-146, January 2022. |
| [9] | Blaser A. R., Ploegmakers I., Benoit M. Acute intestinal failure: International multicenter point of prevalence study // Clin. Nutr. 2020. Vol. 39, No 1. Р. 151–158. Doi: 10.1016/j.clnu.2019.01.005.18. |
| [10] | Mapesa J. O., Maxwell A. L., Ryan E. P. An exposome perspective on environmental enteric dysfunction // Environ. Health Perspect. 2016. Vol. 124, No 8. P. 1121–1126. Doi: 10.1289/ehp.1510459. |
| [11] | Mavlyanov F.Sh., Tursunov S.E., Mavlyanov Sh.Kh., Baratov U. Results of plasty of esophagus atresium in newborn // Thematic journal of Education. Vol-7-Issue Q4- 2022. |
| [12] | Mavlyanov F.Sh., Kamolov S. J. Diagnosis and Treatment of Emergency Abdominal Pathology at the Present Stage // RA JOURNAL OF APPLIED RESEARCH Volume: 08 Issue: 05 May -2022. |
| [13] | Yoseph B. P., Klingensmith N. J., Liang Z. et al. Mechanisms of intestinal barrier dysfunction in sepsis // Shock. 2016. Vol. 46, No 1. Р. 52–59. Doi: 10.1097/ SHK0000000000000565. |
| [14] | Mary et al. Commentary on early enteral feeding versus traditional feeding in neonatal congenital gastrointestinal malformation undergoing intestinal anastomosis: A randomized multicenter controlled trial of an enhanced recovery after surgery (ERAS) component Brindle, Pediatric Surgery, Volume 56, Issue 9, 1485 - 1486. |
| [15] | Peng, Yanfen et al. Early enteral feeding versus traditional feeding in neonatal congenital gastrointestinal malformation undergoing intestinal anastomosis: A randomized multicenter controlled trial of an enhanced recovery after surgery (ERAS) component Journal of Pediatric Surgery, Volume 56, Issue 9, 1479 - 1484. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML