Shomuradova Dilnoza Salimovna1, Jurabekova Aziza Takhirovna2
1Phd, Associate Professor, Department of Neurology, Samarkand State Medical University, Uzbekistan
2Professor Head of the Department of Neurology, Samarkand State Medical University, Uzbekistan
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The study of clinical features of neurological insufficiency in the elderly against the background of thyroid dysfunction seems to be an urgent problem. On the basis of the analysis of the examined patients over 60 years old with thyroid dysfunction, the relationship between the decrease of thyroid hormones production and clinical and neurological disturbances was revealed. It turned out that the lack of thyroid hormones in the elderly changes the clinical picture of the disease, accompanied by more pronounced shifts in cognitive impairment, vestibuloataxic disorder, with a worse prognosis.
Keywords:
Clinical and neurological syndromes, Elderly people, Thyroid dysfunction, Dry skin, Constipation, Asthenization, Weight loss
Cite this paper: Shomuradova Dilnoza Salimovna, Jurabekova Aziza Takhirovna, Complex Interrelationship of Clinical and Neurological Disorders with Thyroid Dysfunction in the Elderly, American Journal of Medicine and Medical Sciences, Vol. 13 No. 4, 2023, pp. 383-387. doi: 10.5923/j.ajmms.20231304.09.
1. Introduction
The issue of the epidemiological situation in relation to thyroid dysfunction in the population, repeatedly becomes the subject of research. For example, screening over 60 years of age, as part of a preventive examination of almost 3,000 people (Framingham Heartstudy), found low thyroid hormone levels in 4% of cases, while high thyroid hormone levels (hyperthyroidism) were found in 9% [1,3]. Other studies by foreign authors, record the prevalence of subclinical thyroid abnormalities in the elderly at about 15-17% (US national study) [4,6]. Most often in old age, signs (hypo and hyperthyroidism) of thyroid dysfunction, are masked under the guise of concomitant somatic diseases or these signs are taken as physiological aging (dry skin, constipation, asthenization, weight loss). Another thing that complicates the diagnosis is the taking of a large number of medications (cardiac blockers, hypotensive, antiarrhythmic), which in turn disturb the symptoms that are classically characteristic of thyroid disorders [2,5]. The gland itself normally should not change its structure with age, and if there is still thyroid dysfunction in the elderly, its main cause is considered to be autoimmune disease (autoimmune thyroiditis) [3,7,8]. Neurological syndromes in the elderly against the background of thyroid deficiency can manifest as neuropathies, again with the need to differentiate neuropathies of diabetic genesis; in the form of coordination disorders, cognitive decline, "age-related" depression. Damage to the nervous system (both central and peripheral) in thyroid deficiency, due to the toxic effects of the thyroid gland, hypersensitivity to catecholamines, and as thyroid hormones affect the synthesis of proteins of the nervous system, on synapses, which primarily depresses the cognitive process. But the most unpredictable change, in principle why it is worth being interested in discovering hypothyroidism, is its complication of all organs and systems, slowing down the metabolic process, the redox process in the body [2,6,7,9]. The central nervous system is very sensitive to thyroid hormone deficiency where there is a violation of the impact of TTG on neurotransmission mechanism (Panchenkova L.A. et al., 2005). As a consequence, a decrease in intelligence, memory, attention, astheno-depressive disorders (Mikhaylova E.B., 2006). Thus, hypothyroidism in old age has a negative impact on health, increasing the risk of dementia, and to identify the pathogenetic mechanisms and interaction of TTH with age, additional research is needed. Consequently, the study of clinical features of neurological insufficiency in the elderly against the background of thyroid dysfunction appears to be an urgent problem.Purpose of the study: to investigate clinical and neurological syndromes in the elderly with thyroid dysfunction.
2. Materials and Methods of Research
In the decree of the President of the Republic of Uzbekistan, on health improvement of the population special attention is paid to the issue of monitoring, entering into the electronic database on the nature of thyroid gland disorders (taking into account iodine deficient region) (2019 PC-4295), based on this a screening program was developed, in which neurologists participated. Patients underwent several stages of screening. At the first stage (routine study) it was necessary to carry out the sampling of the main group for the study, for this purpose all students, during the period of preventive examination, in people over 60 years were taken blood for thyroid hormones; in parallel the state of the thyroid gland was studied by ultrasound examination; the anamnesis of examined by questionnaire was carefully collected. At the second stage, according to TTG, T3,T4 data, Group I was formed - 56 patients with abnormal thyroid hormones, women 41, men 15; Group II - 30 patients. Criteria for inclusion in this group, age over 60 years, absence of cancer and, most importantly, normal levels of thyroid hormones. Patients did not take medications to maintain thyroid function. At this stage, all patients underwent a thorough clinical, neurological and somatic examination. ECG, ultrasound of internal organs, blood biochemistry, MRI (brain, spine in different sections, according to the complaints); cognitive level was studied using neuropsychological scales; neurological examination in the dynamics of examination; paraclinical examinations: blood biochemistry, EEG, UzTDG; patients were examined by an endocrinologist, an ultrasound examination of the thyroid gland was performed, thyroid hormone analysis to diagnose primary hypothyroidism. Neuropsychological examination was used to detect preserved or impaired cognitive and mental function (Hamilton scale, MMSE, frontal dysfunction battery) to control Kerdo autonomic index, in strict order, blood pressure control was performed (day and night). Electroencephalography and electroneuromyography were performed in some cases, if necessary. The study was conducted at the first stage in polyclinics of Samarkand, at the second stage in the therapeutic, neurological departments of the MC SamGMU base, for the period of 2020-2023. The data were statistically processed using the Microsoft Excel program (version 14.0) on an individual computer according to the parameters of Student's statistical method.
3. Results and Their Discussion
Implying old age, everyone understands its inevitability, calmly reacts to the decline in memory, activity. But there are signs of disease that masquerade as old age, thyroid dysfunction. Thyroid hormones regulate metabolism, body weight, are responsible for a person's emotional background. As almost all organs and systems fade in age, the activity of the thyroid gland decreases especially in women. Confirmation of the diagnosis, taking into account the smeared clinical picture, is the clarification of the level of hormones (TSH, T3, T4), ultrasound of the thyroid gland.The research was carried out taking into account the program of preventive examination on health improvement of the population of Uzbekistan (aimed to study thyroid gland function of the population in the zone of iodine deficiency). A planned screening analysis of thyroid hormones of all ages was performed. Initially, sampling was done according to age and corresponding diagnosis (DE). The second stage, an additional examination (ultrasound of the thyroid gland, thyroid hormones, consultation of an endocrinologist) was carried out, made it possible to divide patients with and without thyroid dysfunction. Thus, the main collected group was divided into groups I - patients with DEII degree and without thyroid dysfunction (32), II - patients with DEII degree with thyroid dysfunction (26). For validity of the carried out investigation, the group of volunteers over 65 years old with a relatively favorable health, who underwent preventive dispensary examination at the place of residence (Samarkand) was recruited from outpatient clinics; 20 patients were included into the control group III; only adult population, old age (60 years according to WHO) was studied in our work. According to a routine study, based on blood tests of thyroid hormones (TTG, T3, T4), examination by an endocrinologist, ultrasound of the thyroid gland, patients with thyroid dysfunction were selected, which was approximately 16.3% of the total number examined earlier. Numerous comorbidities in the elderly, require sufficient medications that affect thyroid hormone output. There are medications, such as antiarrhythmic drugs containing iodine, which smoothes the picture, smears the picture with hyperthyroidism. The cause of reduced thyroid dysfunction in the elderly, are anticonvulsant drugs, non-steroidal drugs, glucocorticoid hormones. And since this requires a separate study, this paper only records the medications received, Group I patients, anticoagulants took all one hundred percent, aspirin (American-made) 13 patients, 8 patients before the examination received heparin, in a therapeutic hospital; 5 patients were taking L-dopa; 30 patients were taking Phenibut (which includes Phenobarbital); 2 patients were taking Amiodarone (which improves arrhythmic heart condition); 2 patients were taking Iodomarin (prescribed by an endocrinologist); 1 patient was taking Euthyrox. Consequently, when analyzing thyroid hormones in subclinical forms of the disease, one should consider taking additional drugs in elderly persons. The analysis showed that in elderly patients the incidence of hypothyroidism was much higher than that of hyperthyroidism. Only 3 patients had decreased TTH levels and elevated T4 levels. In all other cases, T4 was decreased and TTH and T3 hormones were elevated (confirming signs of hypothyroidism).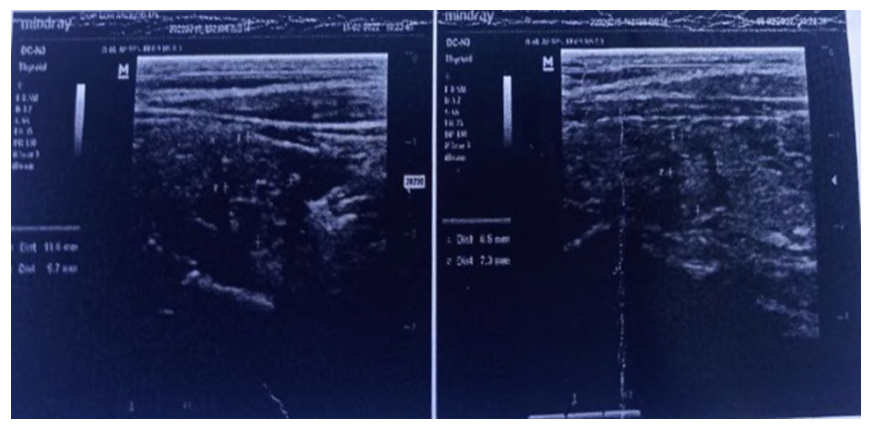 | Figure 1. Patient Memetova Alfiya, born in 1952, nodular goiter with thyroiditis phenomena. hypoplasia of thyroid gland |
For the completeness of reliability of this study, the elderly, examined without signs (or rather without thyroid hormone dysfunction), were offered to continue the examination to identify clinical and neurological syndromes, 30 people gave their consent (in writing), to further stage of the study. Thus, two groups of patients over 60 years of age were formed, Group I patients with thyroid dysfunction, Group II patients without thyroid dysfunction. There were 40 of 47 women in group I, and 25 of 30 in group II.In group. DEII with thyroid dysfunction), primary hypothyroidism due to chronic autoimmune thyroiditis, diffuse nodular goiter, and subclinical (latent) hypothyroidism were identified, where the TTG value was within 6.3±1.9 μME/ml. On average, the TTG value in group II was within 10.5±1.0 µIU/ml, T3 level was 4.1±1.5 pmol/l, T4 level was 6.8±1.4 pmol/l. Examination by an endocrinologist revealed the following symptoms typical for hypothyriosis: rapid fatigability, sleep disturbance (frequent waking up, intermittent, poor falling asleep), swollen face in the morning, increased body weight. The complaints of dizziness, cephalic pain, tinnitus, emotional lability (uncontrollable). From the listed subclinical signs, we can see that they coincide in their variety with the signs of chronic cerebral circulatory disorder (CHD), i.e. the same pattern is traced in Group I (DEII degree without thyroid dysfunction) by the signs: dizziness, headache, asthenoneurotic syndromes. What is the difference? The difference is in the brightness of manifestations of certain syndromes in group II, and in frequency higher. So in Group I headache occurred in 63%, in Group II 93,5%; vestibuloatactic signs 53% and 78,3% respectively; sensory disturbances 15% and 23,7% respectively; pyramidal syndromes in Group I in 30%, and in Group II 47%. Correlation between groups showed that neurological manifestations as chronic circulatory failure prevailed in patients with hypothyroidism. The main complaints of all patients examined were rapid fatigability, poor sleep (or conversely sleepiness), decreased memory, difficulty walking (legs not "docile") in 6 patients of group I; unsteadiness of gait in group I in 17 patients, in group II in 5 patients; complaints of hand tremor were found in 96% of group I cases, in 10 cases in group II. Swelling of limbs and face in 60% of group I and 25% in group II. Complaints of loss of interest in life, emotional lability, tearfulness in 98% of group I, in 5% of group II. Intestinal dysbacteriosis in group I 88.2%, 9% in group II, respectively. Metabolic disorder (excessive body weight) in group I 63% (obesity of 1-2 degrees), 12% in group II, and in parallel in these same patients when studying lipid metabolism, elevated in 71% in group I, 19,9% in group II. Thus, multiphonality of the presented complaints, indicates a vague picture of thyroid dysfunction, occurring under the mask of various symptoms typical for elderly patients. Whereas thyroid hormone indexes in group II patients were initially unchanged, in group I the thyroxine level was reduced in most cases and was 94,200±1,140 nmol/l, (total thyroxine), free was 10,381±0,505 nmol/l, where p<0.001. At the same time the thyroid hormone (THT) content was 2,790±0,360 mI/l, where p<0.001. When considering clinical and neurological signs, we were interested in patients whose complaints raised doubts about uniqueness (weakness in legs, difficulty in walking), conducting differentiation using instrumental, neuroimaging (lumbosacral MRI, ENMG, USG of vessels) methods of investigation, excluded cancer disease, myopathy, though all signs pointed to this process according to the clinic. Electroneuromyography, performed in parallel with thyroid hormone values, showed prolongation of time in tendon reflexes, especially in Achilles reflex. Group I patients had 260.0±5.2 mS, while Group II patients had 350.0±2.9 mS, p<0.001.There is a large body of literature confirming the relationship of thyroid dysfunction in the elderly with clinical symptoms such as cognitive impairment, asthenization. In the examination of patients within the framework of this work, such signs were not an exception. For this purpose, all examinees were offered neuropsychological tests to detect the influence of thyroid hormone disorder on the process of dementia. The gold standard of neuropsychological testing is the MMSE, the "drawing of a clock" test, and the MoCA cognitive assessment scale, which we consider convenient in its use. Thus, according to the results of the correlation between thyroid hormone abnormalities and testing. In group I patients are associated with the right results on all scales. Particularly affected the process of praxis "memorization" among the category of these patients, the average numbers on the MoCA was 11 points, on the MMSE within 15 points, "drawing the clock" corresponded to 1-2 points. These data indicate a moderate degree of cognitive impairment. In group II patients without thyroid hormone abnormalities, MMSE examination was within 20 points, "clock drawing" within 4-5 points, MoCA was 19 points, indicating mild cognitivity associated with age-related vascular disorders. Indicative of clinical signs in the examined patients of Group I were vegetative changes in the form of dry skin, decreased sweating, hair loss (on the scalp, eyebrows) and pronounced edema of the hands and feet. Puffiness of the face appears. Bradycardia up to 60-65 beats per minute is characteristic. In this situation, to clarify the indices, we used Kerdo index determination. The findings confirmed the loss of parasympathetic values in Group I patients. Sympathicotonia prevails (during day and night). Parasympathicotonia was present in 32% of group I patients and in 2% of group II patients during the day and in 11% at night.Symptoms of vestibuloatactic disorders were detected in 6% of Group I patients. These patients noted unsteadiness when walking and standing, gait with legs widely spaced, patients confuse their legs when walking, there was no aggregation, smoothness of movement, the palpation test conducted in patients revealed intension, misses from both hands, while in the control group patients who were found to have coordination disorders, the palpation test was unchanged. That is, Group I patients showed signs of cerebellar insufficiency, which combines impaired coordination, tremor and nystagmus (4%). Thyroid hormone deficiency concomitantly impairs the synthesis of collagen, which is a basic compound in the structure of the spinal disc. Therefore, patients with thyroid dysfunction are more likely to report painful symptoms with mobility in different parts of the spine. And sensory changes develop before motor changes. Damulin I.V. et al. (2011) explain this fact by the deposition of mucopolysaccharides around the peripheral nerves, leading to axonal regeneration against the background of insufficient thyroid hormones. Patients in the main group had pain signs more frequently in 40% of cases than patients in the control group, in 52% there was a decrease in knee reflexes, and during dynamic examination; different levels of reflexes were found, then a complete absence, then medium vividness, then decrease again, in group II there were patients (3 of the whole group) who had diabetes, motor symptoms at the level of tendon reflexes diagnosis revealed their complete stable absence, without any changes in character and symptom, unlike in group I patients The same applies to muscle spasms in the legs, paraesthesia; in group I these signs were more in the proximal parts, symmetrically in both limbs and more often in the daytime, and in group II patients, more often at night and in the distal parts, asymmetrically (only in one limb).The results of the neuroimaging study, indicate a significant role of insufficient thyroid function on the process of progression in the brain. In cases where MRI (or MSCT) is performed, the difference between the comparison groups is found. Dilation of lateral ventricles and dilation of subarachnoid space in group I, was 19.9%, in group II 29.5%; small focal changes of discirculatory nature in group I 30.5%, and in group II 35.5% respectively; leucorrhage indicators in group I 15.7%, in group II 18%; signs of brain substance subtraphy in group I 20%, in group II 31.5% respectively. As can be seen, changes in the structure of the brain according to the stage of dyscirculatory encephalopathy, by age, the worst indicators in patients with a background of hypothyroidism.Level of cognitive and emotional disorders in the examined patients
 |
| |
|
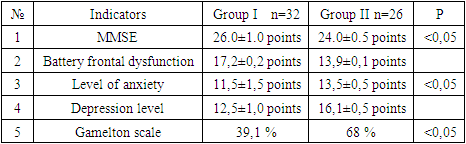
An identical pattern of changes is observed in the examination of the main main vessels of the head on UzTDG. Thus, in group II there was a 2-fold thickening of the intima-media. At the same time, stenosis along the vertebral arteries did not differ significantly in both groups: 23.3% in group I and 25.3% in group II, which reliably confirms the assumption that hemodynamics in the vertebral arteries is directly proportional to the indicators of cervical vertebral shift, which is structurally altered in older patients (but this requires a separate examination), Interesting and important, were the studies of neuropsychological status, with the identification of cognitive impairment. Considering that the examination group (in the general cohort) included patients with DE of II degree, the level of cognitive impairment reflected mild to moderate cognitive dysfunction.Thus, mild cognitive impairment in group II patients with hypothyroidism was detected in 40% of cases and moderate impairment in 60%; in group I the tendency to mild cognitive dysfunction was higher than in moderate impairment; mild cognitive impairment in group I was 38%, and moderate cognitive impairment 36%, and lower than in group II. The MMSE score in group II was 24.0±0.5 and in group I was 26.0±1.0, that is, more severe impairment in the group with hypothyroidism. For a more complete analysis of cognitive dysfunctions, in the examined patients, it was proposed to examine the patients on the "Frontal Dysfunction Battery" test, where the analysis of the results showed, in group I the scores had a range of 17.2±0.2, in group II 13.9±0.1 points; manifestation of spatial process were lower in patients with hypothyroidism. According to the complaints of uncontrollable emotional lability, and the aim of the study was to reveal the emotional sphere in the examined patients, we evaluated the scales data on the level of anxiety and depression in points. The result was as follows: mean score of anxiety level in group II was 13,5±0,5, in group I 11,5±1,5, depression scale was presented in figures of group II 16,1±0,5, in group I 12,5±1,0 respectively. That is, anxiety and depression were more frequently expressed in group II, in patients with hypothyroidism, already at stage II of DE. Hamilton's scale revealed the same indicators, worse in patients with hypothyroidism, in group II depression was found in 68% and in group I 39.1% of cases, where the total score p<0.05. The indicators on EEG (electroencephalography) in the examined groups were insignificant and of little significance. Thus, in Group I patients bioelectrical activity was detected in 40% of cases, and in Group II in 45% (there was virtually no difference between the comparative indices). But in Group II paroxysmal activity was noted in 5 patients, which was not registered in Group I. These indicators are confirmed by data from literary sources (Dubossarskaya SA, 2014; Karr F. et. al 2015, Amonova Z.K. et al. 2022).Thus, hypothyroidism in the elderly, manifests similar clinical and neurological, neuroimaging, neurophysiological and psychological indicators in persons of identical age, but without hypothyroidism. At the same time it has its own features depending on the duration of hypothyroidism, the neurological clinic is more pronounced in its symptomatology, aggravating the process of chronic brain structure. The difficulty of clinical diagnosis lies in the sterile picture of manifestation, which requires doctors to extend diagnostic analysis of the evaluation of patients in old age, the need to include thyroid examination, in the standard program, patients in old age, at the level of control of blood pressure or blood sugar.
4. Conclusions
Based on the analysis of examined patients over 60 years of age with thyroid dysfunction, the relationship of decreased production of thyroid hormones and clinical and neurological disorders has been revealed. The main feature of symptoms associated with thyroid dysfunction is non-specificity, masked in particular in the elderly, where the aging factor is independently represented by chronic impairment of cerebral circulation, disorders of peripheral and autonomic nervous system, rich comorbid background diseases like arterial hypertension, heart, renal and liver failure, diabetes, degenerative disorders of the spine. In spite of this long list of disorders, there is a possibility to detect, in the older generation, the influence of the lack of thyroid hormones on the functional system of the nervous system, which increases in the process of chronic diseases and accelerates the aging of the body, approaching mortality. The differential assessment between elderly groups with thyroid dysfunction and without thyroid hormone disorder, becomes an important prognostic point to be considered in practical gerontology, and the need for further study in this direction. As it can be seen from the above, how much the lack of thyroid hormones in the elderly changes the clinical picture of the disease, accompanied by more pronounced shifts in cognitive impairment, vestibuloataxic disorder, worse prognosis in the issue of neuropathies, up to myopathy syndrome, complexity of this disorder related to diagnosis and treatment, this issue remains controversial judging by the sources of scientific literature.
References
| [1] | Paramonova O.V., Shilova L.N. Hypothyroidism in the elderly - methods of diagnosis and treatment // Medicinal Bulletin № 2 (70). 2018. Vol. 12, pp. 46-53. |
| [2] | Zhitkova Y.V. Cognitive disorders in chronic cerebral ischemia (prospective study) // Dissertation. D., Kazan 2019, 324 p. |
| [3] | Andrea S. Gore, David Crews, Loretta L. Doen, Michelle La Merrill, Heather Patisol, Ami Zota, ScD, "Endocrine-disrupting chemicals (EDCs): An Introduction. A Guide for Public Interest Organizations and Policy Makers." // CVNRES: An Introduction (December 2014), p. 80. |
| [4] | Kotelnikova G.P., Zakharova N.O. Clinical and fundamental aspects of gerontology / / Samara: Samara. State. med. univ., 2015. -399 с. |
| [5] | Hodzhneva D.G., Akhmatova N.R. Thyroid disease and cerebrovascular disease // www.tadqiqot.uz. |
| [6] | Amonova Z.K., Djurabekova A.T. Neuro-Endocrinological Aspects In Patients With Epilepsy // International Conference on Studies in Humanity, Education and SciencesHelsinki, FinlandJanuary 10th2022, p. 115-116. |
| [7] | Jattinder S., Jane A. Franklin Thyroid Disease in the Elderly // https://www.lvrach.ru/1999/10/4528317. |
| [8] | Makar R.D., Makar O.R. Thyroid diseases in old age: features of the clinical course, diagnosis and treatment / Thyroid gland diseases in patients: peculiarities of clinical course, diagnosis and treatment / International Endocrinology Journal 6(12) 2007, http://www.mif-ua.com/archive/article/3779. |
| [9] | Zhukova LA, Gulamov AA, Andreeva NS, Tregubenko EV Evaluation of nosological manifestations of subclinical hypothyroidism and conditions with high-normal levels of thyroid hormone // Modern problems of science and education. - 2017. - № 5. |
| [10] | Shomurodova D.S., Dzhurabekova A.T. Clinical and neurological aspects of thyroid function disturbance in the elderly. // European Journal of Interdisciplinary Research and Development, (2022), 2, 1-6. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML