-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2023; 13(4): 351-354
doi:10.5923/j.ajmms.20231304.02
Received: Feb. 23, 2023; Accepted: Mar. 27, 2023; Published: Apr. 13, 2023

Features of the Postoperative Period in Patients with Acute Appendicitis Depending on the Methods of Surgical Treatment
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKamalov S. J., Mavlyanov F. Sh.
Samarkand State Medical University, Samarkand, Uzbekistan
Correspondence to: Kamalov S. J., Samarkand State Medical University, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2023 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of the study was to identify the features of the course of the postoperative period in patients with destructive forms of acute appendicitis operated on by classical access and laparoscopy. To achieve this goal, in 82 patients with destructive forms of appendicitis admitted to the Samarkand branch of the Republican Research center of emergency medicine in 2021, a comparative analysis of the course of the early postoperative period was carried out. Of these, 41 patients underwent a video-laparoscopic method of treatment and 41 patients underwent an appendectomy using the traditional open method. It has been established that laparoscopic intervention in acute appendicitis is a highly effective method, having the advantages of minimally invasive surgery and quite safe, accompanied by a favorable postoperative period.
Keywords: Appendicitis, Treatment, Laparoscopy, Postoperative period
Cite this paper: Kamalov S. J., Mavlyanov F. Sh., Features of the Postoperative Period in Patients with Acute Appendicitis Depending on the Methods of Surgical Treatment, American Journal of Medicine and Medical Sciences, Vol. 13 No. 4, 2023, pp. 351-354. doi: 10.5923/j.ajmms.20231304.02.
Article Outline
1. Introduction
- Acute appendicitis is the most common surgical disease of the abdominal organs. Destructive forms of acute appendicitis remain an urgent problem of emergency abdominal surgery, due to the rapid development of the inflammatory process in the appendix, atypical clinical manifestations and the difficulty of diagnosis. The percentage of postoperative complications does not decrease either, especially formidable of them are the development of sepsis and multiple organ failure [1].The current stage of development of surgery is characterized by the widespread introduction of various minimally invasive endosurgical technologies into the daily practice of treating patients with emergency pathology. The use of endoscopic surgery in surgical practice is promising and expedient, since it radically improves treatment and improves the quality of life of patients [2].In the treatment of appendicitis, laparoscopy and laparotomy have their own indications and contraindications. The question remains: when is it necessary to switch from laparoscopy to an “open” approach, how justified is it, and will it not worsen the course of the underlying disease? [3].Some endosurgical techniques, primarily laparoscopic appendectomy, have become quite widespread in surgical practice, having proven their effectiveness, however, by far not all authors recognize laparoscopic appendectomy as the unconditional method of choice in the treatment of patients with destructive appendicitis and appendicular peritonitis [4]. Objective: To analyze the features of the course of the postoperative period in patients with destructive forms of acute appendicitis operated on by classical access and laparoscopy.
2. Material and Methods
- A comparative analysis of the course of the early postoperative period was carried out in 82 patients with destructive forms of appendicitis admitted to the Samarkand branch of the Republican Research center of emergency medicine in from January to December 2021. Patients, depending on the method of surgical treatment, were divided into two equal groups. Both groups were comparable in terms of the number of patients, age and gender, and, therefore, it was possible to compare both groups and obtain statistically significant data.The first group consisted of 41 patients who underwent a video laparoscopic method of treatment, the second group also included 41 patients, appendectomy in this group was performed by the traditional open method.All patients underwent a general clinical study of blood, urine, determined the blood group and Rh factor, prothrombin index, blood clotting and bleeding duration using unified methods. With atypical clinical signs of the disease, biochemical blood tests were performed.In all patients with doubtful clinical signs, ultrasound of the abdominal organs, kidneys and urinary system was performed. Ultrasound examinations were carried out on an expert-class ultrasonic device manufactured by Shenzhen Mindray BioMedical (China) model DC-40 full HD, release date 2019 ST7-02000031T, using a 3-10 MHz convex probe, a 4-16 MHz linear probe, and a volumetric probe 1 -8 MHz.To assess the peculiarities of the course of the postoperative period in patients, the following indicators were compared: the severity of the pain syndrome, the need and duration of the use of painkillers, body temperature, the time of activation of the patient in the early postoperative period, as well as the length of stay in the hospital after surgery.Assessing the severity of pain syndrome in patients is a difficult but extremely important task, since treatment tactics depend on it. The severity of pain in the early postoperative period was determined using the Wong-Baker 2008 pain intensity assessment system (Figure 1).
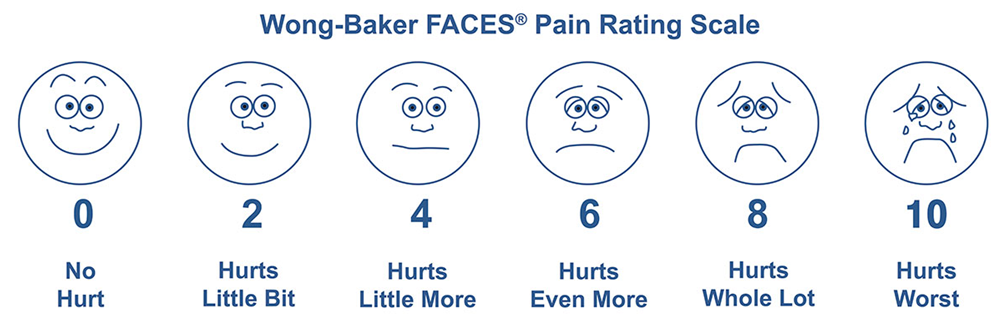 | Figure 1. Wong-Baker scale |
3. Results and Discussions
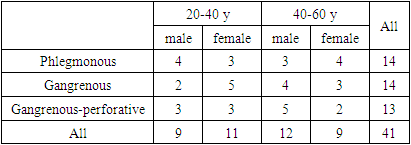
- In the first group of 41 patients intraoperatively phlegmonous form of appendicitis was diagnosed in 14, gangrenous also in 14 and gangrenous-perforative form was detected in 13 patients.The age and sex composition of patients in group 1 is presented in Table 1.
|
|
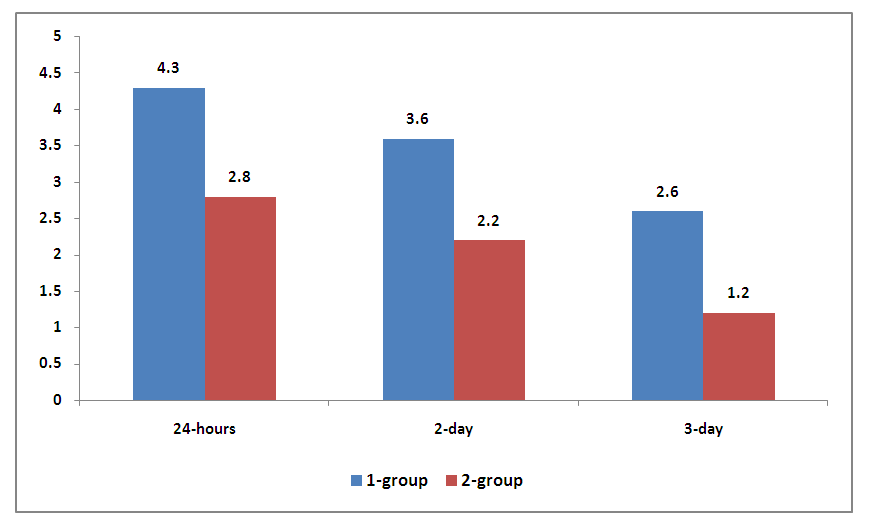 | Figure 2. The average score on the Wong-Baker scale in patients in the immediate postoperative period |
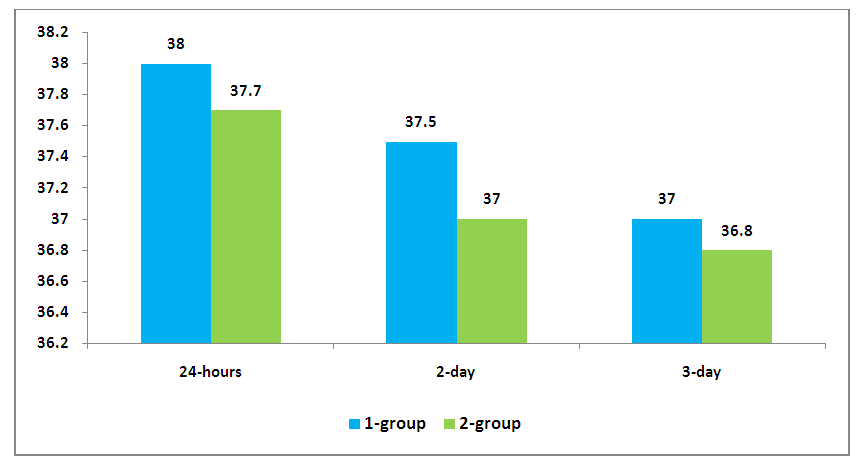 | Figure 3. Indicators of body temperature in patients of groups 1 and 2 |
4. Conclusions
- Thus, based on the advantages of endo-laparoscopic technologies in the diagnosis and treatment of major urgent diseases of the abdominal cavity, in recent years, 63% of the total number of emergency operations for destructive forms of appendicitis were performed by the laparoscopic method. Laparoscopic intervention for acute appendicitis is highly effective, has the advantages of minimally invasive surgery and is quite safe, accompanied by a favorable postoperative period. An endoimaging approach for the treatment of acute appendicitis based on laparoscopic appendectomy should be offered as an alternative to open surgery.
Conflict of Interest
- The authors declare that there is no conflict of interest.
Funding Source
- The was conducted without sponsorship.
Ethics Approval
- The research was approved by the Ethics Committee of the Samarkand state medical university and conducted in accordance with the ethical standards set out in the Helsinki Declaration. All patients received informational consent to conduct the study.